

































































































![Kyste hydatique du foie [enregistrement automatique]](https://cdn.slidesharecdn.com/ss_thumbnails/kystehydatiquedufoieenregistrementautomatique-170224222408-thumbnail.jpg?width=560&fit=bounds)



Publicité
Contenu connexe
Tendances (20)
En vedette (20)


















Publicité
Similaire à Classification pi rads (20)



















Publicité
Classification pi rads
- 1. Classification PI-RADS dans le diagnostic du cancer de la prostate par IRM multiparamétrique Daniel PORTALEZ1,2, Eric BRUGUIERE3 F.Cornud4, R. Renard-Penna5, R. Aziza2, S. Lagarde1, N. Barry Delongchamps4, P. Mozer5, B. Malavaud1 1 3 2 5 4 Hôpital Pitié Salpétrière Hôpital Cochin http://www.prostatecancerassociation.com JFR 2013 1
- 2. OBJECTIFS • 1 - Connaître les séquences IRM utilisées en DETECTION T2, Diffusion, Perfusion • 2 - Connaître les schémas de SECTORISATION de la prostate • 3 – Connaître le score PI-RADS / séquence et GLOBAL • 4 – Savoir rédiger un compte-rendu JFR 2013 10/15/2013 2
- 3. 1 - Les séquences IRM • • • • Séquences T2w Séquence de Diffusion Séquence Dynamique avec Contraste Spectroscopie (optionnelle) Pré-Requis • • • • • JFR 2013 3T (optimum) ou 1,5T ( 0,5T inapproprié) Antenne endorectale: possible Antenne pelvienne phased-array : recommandée Relaxant intestinal : recommandé Injecteur de contraste: recommandé 10/15/2013 3
- 4. 1 - Séquences T2-w axial coronal sagittal Pré-Requis optimum : 3 plans (Axial + sagittal ou Axial + coronal au minimum) Epaisseur : 2,5 -3mm jointives Résolution par plan: 0,5x0,5mm à 1,5T et 0,3x0,3mm à 3T JFR 2013 10/15/2013 4
- 5. 2 - Séquence de Diffusion ADC: b0, 100, 800 DWI b1400 Pré-Requis optimum : Plan axial ≡ plan axial de T2w Epaisseur : 5mm maximum jointives (4mm à 3T) Résolution par plan: 1,5x1,5mm – 2x2mm à 1,5T et 1x1mm à 3T Quantification ADC : au moins 3 valeurs de b avec b max≤800 Séquence « single b » DWI : b1400 ou b 2000 (ratio S/N adéquat) JFR 2013 10/15/2013 5
- 6. 3 - Séquence Dynamique avec Contraste T1 axial Soustraction Pré-Requis optimum : Plan axial ≡ plan axial de T2w Précédée de séquence T1w sans injection (détection d’hématome post-biopsie) Résolution par plan: 0,7x0,7mm – 2x2mm à 1,5T et 0,5x0,5mm à 3T Résolution temporelle maximum : 10-15 s Prolongée jusqu’à 5min pour détecter le wash-out Injecteur de contraste - débit = 3ml/s JFR 2013 10/15/2013 6
- 7. 4 - Spectroscopie Optionnelle : Peut être ajoutée au protocole standard Pré-Requis optimum : Spectroscopie 3D de toute la prostate ( mono-voxel : inapproprié) Taille maximale du voxel : 0,5cm3 Analyse qualitative ou quantitative ( ratios ) JFR 2013 10/15/2013 7
- 8. 2- Sectorisation de la prostate Magnetic Resonance Imaging for the Detection, Localisation, and Characterisation of Prostate Cancer: Recommendations from a European Consensus Meeting Louise Dickinson, Hashim U. Ahmed, Clare Allen, Jelle O. Barentsz, Brendan Carey , Jurgen J. Futterer , Stijn W. Heijmink, Peter J. Hoskin, Alex Kirkham, Anwar R. Padhani, Raj Persad, Philippe Puech, Shonit Punwani, Aslam S. Sohaib, Bertrand Tombal, Arnauld Villers, Jan van der Meulen, Mark Emberton EUROPEAN UROLOGY 59(2011)477–494 JFR 2013 10/15/2013 8
- 9. Le schéma en 16 segments = Minimum Limites: absence de dénomination 2 1 1- Du prolongement antérieur de la zone périphérique 2 - Du stroma fibro-musculaire antérieur JFR 2013 10/15/2013 9
- 10. Le schéma en 27 segments = Optimum Limites: dénomination de la partie postérieure de la zone de transition qui est identique à celle du segment postérieur contigu de la zone périphérique (ex: 3p) La région antérieure débute à 17mm de la surface prostatique postérieure ( longueur d’un échantillon de biopsie). JFR 2013 17mm 10/15/2013 10
- 11. 1- La Base Segments 7p et 1p = Zone Centrale (Mc Neal) Cône glandulaire renversé traversé par les canaux éjaculateurs. Hyposignal physiologique T2 et ADC T2w-Coronal T2w-Axial JFR 2013 Diffusion-ADC 10/15/2013 11
- 12. 1- La Base Segments 1p, 2p et 7p, 8p = Zone Périphérique Hypersignal homogène T2 et ADC Segments 8a et 2a = Zone Périphérique (prolongement antérieur) Hypersignal homogène T2 et ADC T2w-Coronal T2w-Axial JFR 2013 Diffusion-ADC 10/15/2013 12
- 13. 1- La Base Segments 7a et 1a = Zone de Transition (antérieure) Nodule d’hyperplasie bénigne de type glandulaire en hypersignal T2 et ADC, cerné par une capsule en hyposignal T2w-Coronal T2w-Axial JFR 2013 Diffusion-ADC 10/15/2013 13
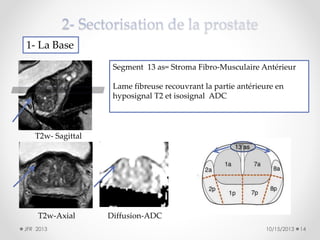
- 14. 1- La Base Segment 13 as= Stroma Fibro-Musculaire Antérieur Lame fibreuse recouvrant la partie antérieure en hyposignal T2 et isosignal ADC T2w- Sagittal T2w-Axial JFR 2013 Diffusion-ADC 10/15/2013 14
- 15. 2- La Partie Moyenne Dans quels segments ? 1- Hyposignal T2, vascularisé, isosignal ADC 2- Hyposignal T2, vascularisé, isosignal ADC T2w-Axial Diffusion-ADC JFR 2013 T1- Dynamique Dynamique Soustraction 3- Hyposignal T2, hypovascularisé, isosignal ADC ? Réponse : 3 diapos suivantes 10/15/2013 15
- 16. 2- La Partie Moyenne T2w-Axial T1- Dynamique Diffusion-ADC 1- Ce nodule d’hyperplasie bénigne de type stromal de contours réguliers est situé dans la partie antérieure et latérale de la zone de transition du lobe droit: 3a Dynamique Soustraction JFR 2013 10/15/2013 16
- 17. 2- La Partie Moyenne T2w-Axial T1- Dynamique Diffusion-ADC 2- Ce nodule d’hyperplasie bénigne de type mixte, glandulaire et stromal est situé dans la partie postérieure de la zone de transition en 3p Dynamique Soustraction JFR 2013 10/15/2013 17
- 18. 2- La Partie Moyenne 3- Stroma fibro-musculaire antérieur du lobe gauche en 14as T2w-Axial T1- Dynamique Diffusion-ADC Dynamique Soustraction JFR 2013 10/15/2013 18
- 19. 3- L’Apex Lésion située à l’apex du lobe droit, dans la partie latérale de la zone périphérique, en 6p. Caractéristiques : hyposignal T2 et ADC, hypersignal b 1400 et hypervascularisée. T2w-Axial Diffusion-ADC JFR 2013 T1-Dynamique Diffusion à b1400 10/15/2013 19
- 20. 3 – Le score PI-RADS • PI-RADS: Prostate Imaging Reporting and Data System: score similaire à celui utilisé en sénologie (BI-RADS en mammographie) dans lequel un score de 1 à 5 est attribué à chaque lésion selon chaque technique mp-MRI : - Score 1: très faible risque de cancer cliniquement significatif Score 2: faible risque Score 3: risque équivoque Score 4: risque élevé Score 5: risque très élevé Cancer cliniquement significatif = Gleason ≥4+3 et/ou lésions ≥ 0,5cm3 en volume ESUR prostate MR guidelines 2012 Jelle O. Barentsz , Jonathan Richenberg , Richard Clements , Peter Choyke , Sadhna Verma , Geert Villeirs , Olivier Rouviere , Vibeke Logager , Jurgen J. Fütterer Eur Radiol (2012) 22:746–757 JFR 2013 10/15/2013 20
- 21. • Score Global PI-RADS (ou ESUR-Score) : score objectif de 3 à 15 obtenu par addition des scores de chacune des 3 techniques mp-MRI recommandées (T2w, Diffusion, Dynamique) pour chaque lésion • Score de LIKERT: score global de 1 à 5 représentant l’intuition personnelle du radiologue du risque de cancer pour chaque lésion indépendamment du score objectif PI-RADS JFR 2013 10/15/2013 21
- 22. Lésion de 10 mm de plus grand axe située en 10p dans la zone périphérique de la partie moyenne du lobe gauche T2: 2/5 Score PI-RADS = 10/15 : risque élevé de cancer Score objectif Echelle de Likert = 3/5 : risque équivoque de cancer ADC: 3/5 Score subjectif Dynamique: 5/5 Courbe de type 3 JFR 2013 Donc… 10/15/2013 22
- 23. Lésion de 10 mm de plus grand axe située en 10p dans la zone périphérique de la partie moyenne du lobe gauche Score PI-RADS = 10/15 : risque élevé de cancer Echelle de Likert = 3/5 : risque équivoque de cancer Etablir un score PI-RADS nécessite de : 1- Localiser chaque lésion dans le secteur correspondant 2- Donner la plus grande dimension de chaque lésion (en mm) sur une coupe axiale en T2 ou en ADC 3- Connaître les images attribuées au score de chaque séquence mp-MRI JFR 2013 10/15/2013 23
- 24. Table 3 PI-RADS scoring system Eur Radiol (2012) 22:746–757 Score Criteria A1. T2WI for the peripheral zone (PZ) 1 Uniform high signal intensity (SI) 2 Linear, wedge shaped, or geographic areas of lower SI, usually not well demarcated 3 Intermediate appearances not in categories 1/2 or 4/5 4 Discrete, homogeneous low signal focus/mass confined to the prostate 5 Discrete, homogeneous low signal intensity focus with extra-capsular extension/invasive behaviour or mass effect on the capsule (bulging), or broad (>1.5 cm) contact with the surface A2. T2WI for the transition zone (TZ) 1 Heterogeneous TZ adenoma with well-defined margins: “organised chaos” 2 Areas of more homogeneous low SI, however well marginated, originating from the TZ/BPH 3 Intermediate appearances not in categories 1/2 or 4/5 4 Areas of more homogeneous low SI, ill defined: “erased charcoal sign” 5 Same as 4, but involving the anterior fibromuscular stroma or the anterior horn of the PZ, usually lenticular or water-drop shaped. Références pour la suite, passer à la diapo suivante B. Diffusion weighted imaging (DWI) 1 No reduction in ADC compared with normal glandular tissue. No increase in SI on any high b-value image (≥b800) 2 Diffuse, hyper SI on ≥b800 image with low ADC; no focal features, however, linear, triangular or geographical features are allowed 3 Intermediate appearances not in categories 1/2 or 4/5 4 Focal area(s) of reduced ADC but iso-intense SI on high b-value images (≥b800) 5 Focal area/mass of hyper SI on the high b-value images (≥b800) with reduced ADC C. Dynamic contrast enhanced (DCE)-MRI 1 Type 1 enhancement curve 2 Type 2 enhancement curve 3 Type 3 enhancement curve +1 For focal enhancing lesion with curve type 2–3 +1 For asymmetric lesion or lesion at an unusual place with curve type 2–3 JFR 2013 24
- 25. LA ZONE PERIPHERIQUE SCORE CRITERIA T2 (Zone Périphérique) 1 Hypersignal uniforme 2 Hyposignal linéaire, triangulaire ou géographique mal défini 3 Apparence intermédiaire entre 1/2 et 4/5 4 Hyposignal discret, homogène, focal/masse limitée à la prostate 5 Hyposignal discret focal avec extension extracapsulaire ou de caractère invasif OU effet de masse sur la capsule (bulging) ou large contact (15 mm) avec la capsule JFR 2013 10/15/2013 25
- 26. SCORE CRITERIA DWI 1 Diffusion et ADC normaux. Pas de réduction d’ADC ni d’hypersignal à b élevé 2 Hypersignal Diffusion + ADC bas sans caractère focal en incluant les anomalies de forme linéaire, triangulaire ou géométrique 3 Apparence intermédiaire entre 1/2 et 4/5 4 ADC bas, focal mais isointense en Diffusion 5 ADC bas et hypersignal Diffusion focal/masse JFR 2013 10/15/2013 26
- 27. SCORE CRITERIA Signal DCE (Dynamique) 1 courbe de type 1 Type 1 2 courbe de type 2 3 courbe de type 3 +1 lésion focale (seulement si type 2-3) Type 2 Type 3 Temps +1 lésion asymétrique OU lésion de localisation inhabituelle (seulement si type 2-3) JFR 2013 10/15/2013 27
- 28. Zone Périphérique PI-RADS = 3 Secteur s 4p, 9p ADC DCE T2 b 1400 Soustraction T2 = 1 Hypersignal uniforme JFR 2013 DWI = 1 Pas de réduction d’ADC ni d’hypersignal en diffusion DCE = 1 Pas d’hypervascularisation focale ou asymétrique 10/15/2013 28
- 29. Zone Périphérique PI-RADS = 4 Secteurs 5p, 11p T2 = 1 DWI = 1 DCE = 2 JFR 2013 10/15/2013 29
- 30. Zone Périphérique Segment 4p T2 = 2 DWI = 2 DCE = 1 JFR 2013 PI-RADS = 5 Secteur 4p , 10p Segment 10p T2 = 2 DWI = 2 DCE = 1 10/15/2013 30
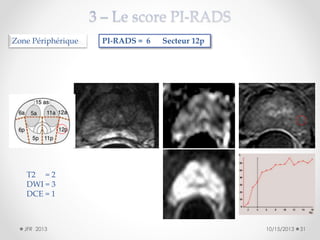
- 31. Zone Périphérique PI-RADS = 6 Secteur 12p T2 = 2 DWI = 3 DCE = 1 JFR 2013 10/15/2013 31
- 32. Zone Périphérique JFR 2013 PI-RADS = 7 Secteur 6p,12p T2 = 2 atténuation de signal linéaires ou géométriques DWI = 2 hypersignal à b 1400 et ADC bas sans lésion focale DCE = 3 courbes de type 3 symétriques 10/15/2013 32
- 33. Zone Périphérique PI-RADS = 8 Secteurs 1p, 2p, 7p, 8p T2 = 3 DWI = 3 DCE = 2 JFR 2013 10/15/2013 33
- 34. Zone Périphérique PI-RADS = 9 Secteur 9p T2 = 2 DWI = 3 DCE = 4 JFR 2013 10/15/2013 34
- 35. Zone Périphérique PI-RAD = 9 Secteur 4p et = 5 Secteur 10p T2 = 2 et 2 atténuations linéaires DWI = 2 et 2 faible atténuation ADC , sans anomalie à b1400 DCE = 5 et 1 courbes de type 3 à droite et de type 1 à gauche JFR 2013 10/15/2013 35
- 36. Zone Périphérique PI-RADS = 10 Secteurs 2p, 10p 2p 10p Segment 2p JFR 2013 T2 = 3 DWI = 2 DCE = 5 Segment 10p T2 = 2 DWI = 3 DCE = 5 10/15/2013 36
- 37. Zone Périphérique PI-RADS = 11 Secteur 1p T2 = 4 DWI = 4 DCE = 3 JFR 2013 10/15/2013 37
- 38. Zone Périphérique PI-RADS = 12 Secteur 1p T2 = 4 DWI = 5 DCE = 3 JFR 2013 10/15/2013 38
- 39. Zone Périphérique T2 PI-RADS = 13 Secteur 6p = 4 masse en hyposignal DWI = 5 ADC bas ( 0,693) et hypersignal à b 1400 DCE = 4 Courbe de type 2 +1 (focale) +1 (asymétrique) JFR 2013 10/15/2013 39
- 40. Zone Périphérique PI-RADS = 14 Secteur 8p T2 = 4 DWI = 5 DCE = 5 JFR 2013 10/15/2013 40
- 41. Zone Périphérique PI-RADS = 15 Secteurs 5p, 6p T2 = 5 DWI = 5 DCE = 5 JFR 2013 10/15/2013 41
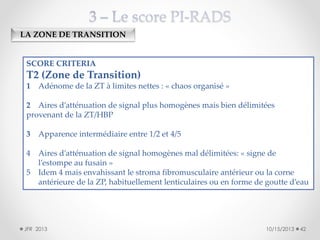
- 42. LA ZONE DE TRANSITION SCORE CRITERIA T2 (Zone de Transition) 1 Adénome de la ZT à limites nettes : « chaos organisé » 2 Aires d’atténuation de signal plus homogènes mais bien délimitées provenant de la ZT/HBP 3 Apparence intermédiaire entre 1/2 et 4/5 4 Aires d’atténuation de signal homogènes mal délimitées: « signe de l’estompe au fusain » Idem 4 mais envahissant le stroma fibromusculaire antérieur ou la corne antérieure de la ZP, habituellement lenticulaires ou en forme de goutte d’eau 5 JFR 2013 10/15/2013 42
- 43. Zone de Transition PI-RADS = 3 T2 = 1 DWI = 1 DCE = 1 JFR 2013 10/15/2013 43
- 44. Zone de Transition PI-RADS = 4 T2 = 2 DWI = 1 DCE = 1 JFR 2013 b 2000 10/15/2013 44
- 45. Zone de Transition Secteur 3a T2 = 3 DWI = 2 DCE = 1 JFR 2013 PI-RADS = 6 Secteur 3a = 5 Secteur 9p Secteur 9p T2 = 2 DWI = 2 DCE = 1 10/15/2013 45
- 46. Zone de Transition PI-RADS = 7 Secteur 3a = 5 Secteur 9p Secteur 14as T2 = 5 DWI = 3 DCE = 1 JFR 2013 10/15/2013 46
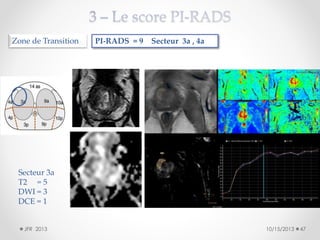
- 47. Zone de Transition PI-RADS = 9 Secteur 3a , 4a Secteur 3a T2 = 5 DWI = 3 DCE = 1 JFR 2013 10/15/2013 47
- 48. Zone de Transition PI-RADS = 10 Secteur 11a T2 = 4 DWI = 5 DCE = 1 JFR 2013 10/15/2013 48
- 49. Zone de Transition PI-RADS = 11 Secteurs 5a, 5p T2 = 4 DWI = 3 DCE = 4 JFR 2013 10/15/2013 49
- 50. Zone de Transition PI-RADS = 12 Secteur 3a T2 = 4 DWI = 5 DCE = 3 JFR 2013 10/15/2013 50
- 51. Zone de Transition PI-RADS = 13 Secteur 15as T2 = 5 DWI = 4 DCE = 4 JFR 2013 10/15/2013 51
- 52. Zone de Transition PI-RADS = 14 Secteur 4a T2 = 5 DWI = 4 DCE = 5 JFR 2013 10/15/2013 52
- 53. Zone de Transition PI-RADS = 15 Secteurs 3a, 9a, 14as T2 = 5 DWI = 5 DCE = 5 JFR 2013 10/15/2013 53
- 54. PONDERATION DU SCORE PI-RADS 1- En Zone Périphérique, DWI prépondérante pour le diagnostic 2- En Zone de Transition, T2-w prépondérante pour le diagnostic 3- Score de Likert 1 à 5 : avis subjectif du radiologue JFR 2013 10/15/2013 54
- 55. PONDERATION DU SCORE PI-RADS 1- En Zone Périphérique, DWI prépondérante pour le diagnostic T2 = 2 DWI = 3 DCE = 1 Total PI-RADS 6 JFR 2013 PONDERATION: Likert 3 = majoration du degré de suspicion car DWI > T2 et DCE 10/15/2013 55
- 56. PONDERATION DU SCORE PI-RADS 2- En Zone de Transition, T2-w prépondérante pour le diagnostic JFR 2013 T2: score 5 DWI: score 3 DCE: score 1 Total: PI-RADS 9 PONDERATION: Likert 4 = majoration du degré de suspicion car T2 très suspect 10/15/2013 56
- 57. 4- Le Compte-Rendu Exemple N°1 Page 1 JFR 2013 10/15/2013 57
- 58. Exemple N°1 Page 2 JFR 2013 4- Le Compte-Rendu 10/15/2013 58
- 59. 4- Le Compte-Rendu Exemple N°2 Page 1 JFR 2013 10/15/2013 59
- 60. 4- Le Compte-Rendu Exemple N°2 Page 2 JFR 2013 10/15/2013 60
- 61. MEMENTO : critères ESUR de lecture d’IRM multiparamétrique JFR 2013 10/15/2013 61
- 62. MEMENTO : Séquence T2 pour la ZP 1/5 Hypersignal normal Nodule d’hyperplasie bénin (encapsulé, en hypersignal) JFR 2013 2/5 Hyposignal linéaire 3/5 4/5 5/5 Masse focale en hyposignal, limitée à la prostate Extension extracapsulaire 62
- 63. MEMENTO : Séquence T2 pour la ZT 1/5 Hypersignal homogène, bien limité (capsule périphérique) 2/5 Hyposignal bien limité, avec capsule périphérique 3/5 4/5 5/5 Hyposignal plus homogène, mal délimité « effacé au fusain » Corne antérieure de la ZP Lésion en hyposignal du SFMA JFR 2013 63
- 64. MEMENTO : Séquence de Diffusion (ZP et ZT) 1/5 ADC et diffusion normaux JFR 2013 2/5 ADC bas Diffusion Hyper Caractère diffus 3/5 Hyposignal sur l’ADC petit ou valeur d’ADC peu abaissée 4/5 ADC bas Diffusion ISO Caractère focal 5/5 ADC bas Diffusion HYPER Caractère focal 64
- 65. MEMENTO : Séquence de Perfusion (ZP et ZT) 1/5 Courbe type 1 2/5 Courbe type 2 Symétrique Non focale 3/5 Courbe type 2 Asymétrique Non focale Courbe type 3 Symétrique Non focale JFR 2013 4/5 Courbe type 2 Focale Asymétrique 5/5 Courbe type 3 Focale Asymétrique Courbe type 3 Asymétrique Non focale 65
- 66. Conclusion • 1- Systématiser la technique (durée 18 min- 24min) • 2- Systématiser l’Interprétation: Lecture indépendante de chaque séquence Lecture inter-dépendante des 3 séquences Score de chaque cible / séquence et global Mesure de chaque cible (+ grand diamètre en T2/DWI) Localisation de chaque cible dans le(s) secteurs • 3- Systématiser le compte-rendu http://www.prostatecancerassociation.com JFR 2013 10/15/2013 66
- 67. Répondre aux Deux Cas Cliniques JFR 2013 10/15/2013 67
- 68. Cas Clinique N°1 Né le 21/06/1949 PSA = 4,5ng/ml en progression TR: fermeté du lobe gauche Séquence T2 axiale 10mm JFR 2013 10/15/2013 68
- 69. Cas Clinique N°1 Diffusion: DWI Cartographie ADC à b0, b100 et b800 ADC= 1,01 10mm JFR 2013 10/15/2013 69
- 70. Cas Clinique N°1 DIFFUSION (DWI) single b b 2000 JFR 2013 10/15/2013 70
- 71. Cas Clinique N°1 Cible Symétrique 2 ROI’s placés l’un dans la cible, l’autre en position symétrique PERFUSION(DCE) Délai: 42 sec après injection JFR 2013 10/15/2013 71
- 72. Cas Clinique N°1 Donner ci-dessous votre réponse Secteur Dimension (en mm) Score T2 Score DWI Score DCE PI-RADS Likert Cible 1 Cible 2 Cible 3 JFR 2013 10/15/2013 72
- 73. Cas Clinique N°2 77 ans, PSA = 15 ng/ml en progression, TR: normal Séquence T2 axiale JFR 2013 10mm 10/15/2013 73
- 74. Cas Clinique N°2 ADC Sagittale T2 JFR 2013 ROI: Valeurs ADC T2 Diffusion b800 Perfusion soustraite T1 natif 10/15/2013 74
- 75. Cas Clinique N°2 Perfusion Perfusion soustraite JFR 2013 10/15/2013 75
- 76. Cas Clinique N°2 Donner ci-dessous votre réponse Secteur Dimension (en mm) Score T2 Score DWI Score DCE PI-RADS Likert Cible 1 Cible 2 Cible 3 http://www.prostatecancerassociation.com JFR 2013 10/15/2013 76