



























































More Related Content
Similar to Art of predicting root coverage in localized gingival recession (20)
More from Shimaa Hussein Kotb (11)



![Oral health is a gate for systemic health [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/oralhealthisagateforsystemichealthautosaved-240102155231-f6ff474b-thumbnail.jpg?width=560&fit=bounds)
![Oral health is a gate for systemic health [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/oralhealthisagateforsystemichealthautosaved-231224185950-e72836d5-thumbnail.jpg?width=560&fit=bounds)




Recently uploaded (20)




















Art of predicting root coverage in localized gingival recession
- 1. The Art of predicting Root Coverage in Localized Gingival Recession. Tips & Tricks?! prepared by Dr. Shimaa Kotb Assistant lecturer of Oral Medicine, Periodontology, Oral Diagnosis & Dental Radiology Sphinx University
- 3. A charming smile • The key to facial attractiveness. • Modern dentistry concerned with patients, esthetic expectation.
- 4. Periodontal defect Compromised esthetics & disturb patient, challenging to clinician. .
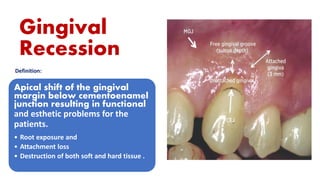
- 5. Gingival Recession Definition: Apical shift of the gingival margin below cementoenamel junction resulting in functional and esthetic problems for the patients. • Root exposure and • Attachment loss • Destruction of both soft and hard tissue .
- 6. Clinical Significance Exposed roots susceptible to: ❑Hypersensitivity ❑Root Caries ❑Oral hygiene problems ❑Plaque accumulation ❑Compromised esthetics
- 7. Multifactorial complex causes. Bacterial is the main cause, associated e predisposing factors.
- 8. Classification systems of gingival recession Aim: ▪ Provide a framework to aid in accurate diagnosis of the condition so the dentist can easily predict prognosis and treatment outcomes.
- 9. Classification of Gingival Recession 1.Sullivan and Atkins (1968) according recession depth& width. .Shallow narrow .Shallow wide .Deep narrow .Deep wide
- 10. Classification of Gingival Recession Bengue et al classification 1983 According Number of teeth affected & coverage prognosis: ❑Generalized • U –shaped (Periodontal diseases) poor ❑Localized • V –shaped (traumatic occlusion)fair • I –shaped (good)
- 11. Class I ▪ Marginal tissue recession, not extend to MGJ. ▪There is no bone or soft tissue loss in the inter- dental area. ▪100% root coverage can be anticipated. Class II ▪ Marginal tissue recession, extends to MGJ. ▪ There is no bone or soft tissue loss in the inter-dental area. ▪ 100% root coverage can be anticipated. Miller classification1985 Depend on extent of defect & relation to MGJ/ KT.
- 12. Miller classification1985. Class III ▪ Marginal tissue recession, extends to MGJ. ▪ Bone or soft tissue loss in inter-dental area is present, or there is mal-position of the teeth, which prevents the attempting of 100% of root coverage. ▪ Partial root coverage can be anticipated.
- 13. Class IV ▪ Marginal tissue recession, extends to MGJ. ▪ The bone or soft tissue loss in the inter- dental area ▪ and/or mal-position of teeth is so severe, ▪ root coverage cannot be anticipated. Miller classification1985
- 14. Advantage of Miller classification Depend on : Morphological evaluation of the periodontal defect clinically. Evaluate the position of gingival margin in relation to the two adjacent teeth (if adjacent teeth missing, diagnosis become difficult) useful in predicting amount of root coverage following graft procedure.
- 15. Limitation of Miller classification No information about keratinized tissue. Difficulty in locating MGJ. Confusion in identifying Miller’s Class I and II. A lack of distinct criteria (measure the soft/hard tissue loss in the interproximal area).
- 16. Limitation of Miller classification Can,t classify recession in palatal surface due to lack MGJ palatal side. No identification between class III & IV, if no adjacent teeth present. Recession interdental papillae not classified according to miller classification.
- 17. New classification…....Cairo et al. 2011 according to interdental attachment loss Explained the grey areas between the Miller classes. Re-organized GR classes based on the interproximal attachment level. used as a reliable parameter to determine bone loss.
- 18. Cairo et al Classification GRT1: no interdental attachment loss. The interdental CEJ is not detectable clinically. (Miller Class I and II). GRT2: interdental attachment loss less than or equal to buccal attachment loss. (Miller Class III) GRT3: interdental attachment loss higher than buccal attachment loss. (Miller Class IV)
- 19. Predictability of treatment outcomes Depend on “Prognosis Keys” Depend on: 1.Defect Factor 2. Patient Factors 3. Operator Factor
- 21. Prognosis Recession Size: the wider the recession, the more challenging it. Amount of keratinized tissue sufficient amount facilitates its stabilization during suturing) (good prognosis) Papillae dimension:crucial predictor factor of root coverage outcomes & Which affect vascular bed for surgical papilla of the covering flap. Papilla height ≥5 mm is associated with CRC. Tooth malposition (rotation) change dimensions of interproximal papilla even without presence of CAL. Prognosis (Gingiva related factor)
- 23. Prognosis related to operator Depend on Individual skills & Experience
- 24. Management
- 25. Management •Mechanical debridement of microbial biofilm. •Meticulous Oral Hygiene instruction. •Remove overhang subgingival restoration. •High fluoride Application for dentin hypersensitivity Non-surgical Management
- 26. Management … Surgical approach Root coverage surgery (Muco-gingival surgery) Plastic surgical correction of gingiva. Surgery divided into: Flap + graft technique
- 28. Management • Flap Design: • Coronally positioned flap • laterally positioned flap • Semilunar pedicle flap • Pouch and tunnel flap • Graft types: • Free gingival graft • connective tissue graft • Subepithelial connective tissue graft • Guided tissue regeneration tech. Surgical
- 31. References ❑ Amine, K., Kholti, W. E., & Kissa, J. (2019). Periodontal root coverage. https://doi.org/10.1007/978-3-030-20091-6 ❑ Pini-Prato, G. The Miller classification of gingival recession: Limits and drawbacks. J. Clin. Periodontol. 2011, 38, 243–5. ❑ Imber, Jean-Claude, and Adrian Kasaj. "Treatment of gingival recession: when and how?." International dental journal 2021; 71.3: 178-87. ❑ Fageeh, H.I.; Fageeh, H.N.; Bhati, A.K.; Thubab, A.Y.; Sharrahi, H.M.H.; Aljabri, Y.S.; et al. Assessing the Reliability of Miller’s Classification and Cairo’s Classification in Classifying Gingival Recession Defects: A Comparison Study. Medicina 2024, 60, 205. ❑ Stimmelmayr M, Allen EP, Gernet W, Edelhoff D, Beuer F, Schlee M,et al . Treatment of gingival recession in the anterior mandible using the tunnel technique and a combination epithelialized-subepithelial connective tissue graft-a case series. Int J Periodontics Restorative Dent. 2011 Apr;31(2):165-73. ❑ Weinberg E, Kolerman R, Kats L, Cohen O, Masri D, Sebaoun A, Slutzkey G. Coronally Advanced Flap with Connective Tissue Graft for Treating Orthodontic-Associated Miller Class III Gingival Recession of the Lower Incisors: A One-Year Retrospective Study. J Clin Med. 2022 Jan 1;11(1):235. ❑ Kotb, S.; Maged, M.; Fouad Edrees, M. Predictability of Maximum Root Coverage in Muco-Plastic Surgery of Localized Gingival Recession. Preprints 2024, 2024111434.
- 32. Thank You