Hiv guideline who 2010
1 like912 views

This document provides recommendations for antiretroviral therapy (ART) for HIV-infected adults and adolescents in a public health approach. It was revised in 2010 by the World Health Organization with input from experts and institutions around the world. The recommendations aim to provide guidance on when to start ART, what first- and second-line regimens to use, and how to monitor patients and provide additional care interventions. The guidelines emphasize simplified and standardized approaches to optimize access to treatment and promote adherence and retention in low-resource settings.


















































![43
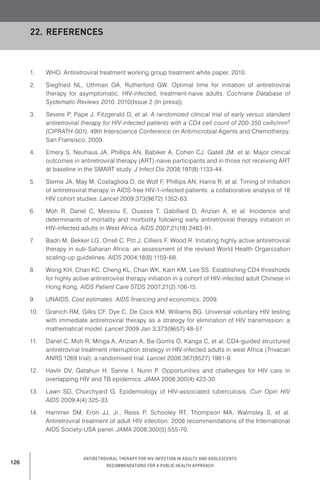
Table 11. ART regimens recommended for women with prior exposure to
PMTCT regimen
Previous ARV exposure for PMTCT Recommendations for initiation of
ART when needed for treatment
of HIV for maternal health
sdNVP1 (+/- antepartum AZT) with
no AZT/3TC tail2 in last 12 months
Initiate a non-NNRTI regimen
PI preferred over 3 NRTI
sdNVP (+/- antepartum AZT) with
an AZT/3TC tail in last 12 months
Initiate an NNRTI regimen
If possible, check viral load3 at 6 months
and if >5000 copies/ml, switch to second-
line ART with PI
sdNVP (+/- antepartum AZT) with or without
an AZT/3TC tail over 12 months ago
Initiate an NNRTI regimen
If possible, check viral load3 at 6 months
and if >5000 copies/ml, switch to second-
line ART with PI
Option A4
Antepartum AZT (from as early as 14 weeks
of gestation)
sdNVP at onset of labour*
AZT + 3TC during labour and delivery*
AZT + 3TC tail for 7 days postpartum*
* sd-NVP and AZT + 3TC can be omitted if
mother receives >4 weeks of AZT
antepartum
Initiate an NNRTI regimen
If possible, check viral load3 at 6 months
and if >5000 copies/ml, switch to second-
line ART with PI
If no sdNVP was given, start standard
NNRTI (viral load does not need to be
checked unless clinically indicated as no
sdNVP received)
All triple ARV regimens (including Option B),
irrespective of duration of exposure and time
since exposure
Option B4
Triple ARV from 14 weeks gestation until
after all exposure to breast milk has ended
AZT + 3TC + LPV/r
AZT + 3TC + ABC
AZT + 3TC + EFV
TDF + [3TC or FTC] + EFV
Initiate standard NNRTI regimen
If EFV-based triple ARV was used for
prophylaxis and no tail (AZT + 3TC; or TDF
+ 3TC; or TDF + FTC) was given when triple
ARV was discontinued after cessation of
breastfeeding (or delivery if formula
feeding), check viral load3 at 6 months and
if >5000 copies/ml, switch to second-line
ART with PI
1Single-dose nevirapine (sdNVP) is one 200-mg tablet of NVP.
2A tail is the provision of two NRTIs, typically AZT/3TC, for a minimum of 7 days following sdNVP or the cessation of
any NNRTI-based regimen with the objective of minimizing NNRTI resistance.
3If VL is not available, continue NNRTI regimen and monitor clinically (and immunologically if available).
4Options A or B are viewed as equally effective for PMTCT in women who do not require therapy for their own health
and are recommended options in the 2010 update of Use of antiretroviral drugs for treating pregnant women and
preventing HIV infection in infants.](https://image.slidesharecdn.com/hivguidelinewho2010-120120093817-phpapp02/85/Hiv-guideline-who-2010-51-320.jpg)




![48
Antiretroviral therapy for HIV infection in adults and adolescents
Recommendations for a public health approach
16.1. Recommendations
1. Where available, use viral load (VL) to confirm treatment failure.
(Strong recommendation, low quality of evidence)
2. Where routinely available, use VL every 6 months to detect viral replication.
(Conditional recommendation, low quality of evidence)
3. A persistent VL of >5000 copies/ml confirms treatment failure.
(Conditional recommendation, low quality of evidence)
4. When VL is not available, use immunological criteria to confirm clinical failure.
(Strong recommendation, moderate quality of evidence)
In making these recommendations, the panel was concerned by the limitations of clinical and
immunological monitoring for diagnosing treatment failure, and placed high value on avoiding
premature or unnecessary switching to expensive second-line ART. The panel also valued the
need to optimize the use of virological monitoring and ensure adherence.
16.2. Evidence
A systematic review was conducted to assess different strategies for determining when to switch
antiretroviral therapy regimens for first-line treatment failure among PLHIV in low-resource
settings. Standard Cochrane systematic review methodology was employed. Outcomes of
interest in order of priority were mortality, morbidity, viral load response, CD4 response and the
development of antiretroviral resistance.
16.3. Summary of findings
Based on the pooled analysis of the side-effects from two randomized trials (Home-based AIDS
care [HBAC] and Development of antiretroviral therapy in Africa [DART]), clinical monitoring
alone (compared to combined immunological and clinical monitoring or to combined virological,
immunological and clinical monitoring) resulted in increases in mortality, disease progression
and unnecessary switches, but there were no differences in serious adverse events.(148,149)
However, in the HBAC trial, combined immunological and clinical monitoring was compared to
combined virological, immunological and clinical monitoring, and there were no differences in
mortality, disease progression, unnecessary switches or virological treatment failures.(148)
Viral load measurement is considered a more sensitive indicator of treatment failure compared
to clinical or immunological indicators. VL may be used in a targeted or routine strategy. The
objective of the targeted strategy is to confirm suspected clinical or immunological failure,
maximizing the clinical benefits of first-line therapy and reducing unnecessary switching to
second-line therapy. Targeted VL may also be used earlier in the course of ART (within 4 to 6
months of ART initiation) to assess adherence and introduce an adherence intervention in at-risk
patients before viral mutations start to accumulate.(150)
16. When to switch ART](https://image.slidesharecdn.com/hivguidelinewho2010-120120093817-phpapp02/85/Hiv-guideline-who-2010-56-320.jpg)











































![92
Antiretroviral therapy for HIV infection in adults and adolescents
Recommendations for a public health approach
WhatARTtostart
Authors: GeorgeRutherford,AlicenSpauldin
Date: 8Oct2009
Question: ShouldEFVvsNVPbeusedforinitialART?(Randomizedclinicaltrials)
Settings: Multiplelocations
Bibliography: 1.AyalaGaytanJJ,delaGarzaERZ,GarciaMC,ChavezSBV.Nevirapineorefavirenzincombinationwithtwo
nucleosideanaloguesinHIVinfectedantiretroviralnaivepatients.MedInternMex2004;20:24.2.ManosuthiW,
SungkanuparphS,TantanathipP,LueangniyomkulA,MankatithamW,PrasithsirskulW,BuraptarawongS,Thongyen
S,LikanonsakulS,ThawornwaU,PrommoolV,KuxrungthamK,2NRStudyTeam.Arandomizedtrialcomparing
plasmadrugconcentrationsandefficaciesbetween2nonnucleosidereverse-transcriptaseinhibitor-basedregimens
inHIV-infectedpatientsreceivingrifampicin:theN2RStudy.ClinInfectDis2009;48:1752-9.3.NúñezM,SorianoV,
Martín-CarboneroL,BarriosA,BarreiroP,BlancoF,García-BenayasT,González-LahozJ.SENC(SpanishEfavirenz
vs.NevirapineComparison)trial:arandomized,open-labelstudyinHIV-infectednaiveindividuals.HIVClinTrials
2002;3:186-94.4.SowPG,BadianeM,DialloPD,LoI,NdiayeB,GayeAM.Efficacyandsafetyof
lamivudine+zidovudine+efavirenzandlamivudine+zidovudine+névirapineintreatmentHIV1infectedpatients.A
rétrospectivecrossstudyanalysis[AbstractCDB0584].XVIInternationalAIDSConference,Toronto,Canada,13−18
August2006.5.vandenBerg-WolfM,HullsiekKH,PengG,KozalMJ,NovakRM,ChenL,CraneLR,MacarthurRD;
CPCRA058StudyTeam,theTerryBeirnCommunityProgramsforClinicalResearchonAIDS(CPCRA),andThe
InternationalNetworkforStrategicInitiativeinGlobalHIVTrials(INSIGHT).Virologic,immunologic,clinical,safety,
andresistanceoutcomesfromalong-termcomparisonofefavirenz-basedversusnevirapine-basedantiretroviral
regimensasinitialtherapyinHIV-1-infectedpersons.HIVClinTrials2008;9:324-36.6.vanLethF,KappelhoffBS,
JohnsonD,LossoMH,Boron-KaczmarskaA,SaagMS,HallDB,LeithJ,HuitemaAD,WitFW,BeljnenJH,LangeJM;
2NNStudyGroup.Pharmacokineticparametersofnevirapineandefavirenzinrelationtoantiretroviralefficacy.AIDS
ResHumRetroviruses2006;22:232-39.](https://image.slidesharecdn.com/hivguidelinewho2010-120120093817-phpapp02/85/Hiv-guideline-who-2010-100-320.jpg)


![95
Authors:GeorgeRutherford,AlicenSpaulding
Date:8Oct2009
Question:ShouldEFVvsNVPbeusedforinitialART?(observationalstudies)
Settings:Multiplelocations
Bibliography:1.AnnanT,MandaliaS,BowerM,GazzardB,NelsonM.Theeffectofyearoftreatmentandnucleosideanalogue
backboneondurabilityofNNRTIbasedregimens[AbstractWePe12.2C03].3rdConferenceonHIVPathogenesisandTreatment,Rio
deJaneiro,Brazil,24-27July2005.2.AranzabalL,CasadoJL,MoyaJ,QueredaC,DizS,MorenoA,MorenoL,AntelaA,Perez-Elias
MJ,DrondaF,MarínA,Hernandez-RanzF,MorenoA,MorenoS.Influenceofliverfibrosisonhighlyactiveantiretroviraltherapy-
associatedhepatotoxicityinpatientswithHIVandhepatitisCviruscoinfection.ClinInfectDis2005;40:588-93.3.AurpibulL,Puthanakit
T,LeeB,MangklabruksA,SirisanthanaT,SirisanthanaV.LipodystrophyandmetabolicchangesinHIV-infectedchildrenonnon-
nucleosidereversetranscriptaseinhibitor-basedantiretroviraltherapy.AntivirTher2007;12:1247-54.4.BannisterWP,RuizL,Cozzi-
LepriA,MocroftA,KirkO,StaszewskiS,LovedayC,KarlssonA,MonforteA,ClotetB,LundgrenJD.Comparisonofgenotypic
resistanceprofilesandvirologicalresponsebetweenpatientsstartingnevirapineandefavirenzinEuroSIDA.AIDS2008;22:367-76.5.
BerenguerJ,BellonJM,MirallesP,AlvarezE,CastilloI,CosinJ,LopezJC,SanchezCondeM,PadillaB,ResinoS.Association
betweenexposuretonevirapineandreducedliverfibrosisprogressioninpatientswithHIVandhepatitisCviruscoinfection.ClinInfect
Dis2008;46:137-43.6.BoulleA,OrrelC,Kaplan,VanCutsemG,McNallyM,HilderbrandK,MyerL,EggerM,CoetzeeD,MaartensG,
WoodR.Substitutionsduetoantiretroviraltoxicityorcontraindicationinthefirst3yearsofantiretroviraltherapyinalargeSouth
Africancohort.AntivirTher2007;12:753-60.7.BoulleA,VanCutsemG,CohenK,HilderbrandK,MatheeS,AbrahamsM,Goemaere
E,CoetzeeD,MaartensGT.Outcomesofnevirapine-andefavirenz-basedantiretroviraltherapywhencoadministeredwithrifampicin-
basedantituberculartherapy.JAMA2008;300:530-9.8.BraithwaiteRS,KozalMJ,ChangCC,RobertsMS,FultzSL,GoetzMB,Gibert
C,Rodriguez-BarradasM,MoleL,JusticeAC.Adherence,virologicalandimmunologicaloutcomesforHIV-infectedveteransstarting
combinationantiretroviraltherapies.AIDS2007;21:1579-89.9.deBeaudrapP,EtardJF,GuèyeFN,GuèyeM,LandmanR,GirardPM,
SowPS,NdoyeI,DelaporteE;ANRS1215/1290StudyGroup.Long-termefficacyandtoleranceofefavirenz-andnevirapine-containing
regimensinadultHIVtype1Senegalesepatients.AIDSResHumRetroviruses2008;24:753-60.10.EnaJ,AmadorC,BenitoC,Fenoll
V,PasquauF.Riskanddeterminantsofdevelopingseverelivertoxicityduringtherapywithnevirapine-andefavirenz-containing
regimensinHIV-infectedpatients.IntJSTDAIDS2003;14:776-81.11.GeorgeC,YesodaA,JayakumarB,LalL.Aprospectivestudy
evaluatingclinicaloutcomesandcostsofthreeNNRTI-basedHAARTregimensinKerala,India.JClinPharmTher2009;34:33-40.12.
HartmannM,WitteS,BrustJ,SchusterD,MosthafF,ProcacciantiM,RumpJA,KlinkerH,PetzoldtD.Comparisonofefavirenzand
nevirapineinHIV-infectedpatients(NEEFCohort).IntJSTDAIDS2005;16:404-9.13.KeiserP,NassarN,WhiteC,KoenG,MorenoS.
Comparisonofnevirapine-andefavirenz-containingantiretroviralregimensinantiretroviral-naïvepatients:acohortstudy.HIVClin
Trials2002;3:296-303.14.MadecY,LaureillardD,PinogesL,FernandezM,PrakN,NgethC,MoeungS,SongS,BalkanS,Ferradini](https://image.slidesharecdn.com/hivguidelinewho2010-120120093817-phpapp02/85/Hiv-guideline-who-2010-103-320.jpg)


![98
Antiretroviral therapy for HIV infection in adults and adolescents
Recommendations for a public health approach
Authors: GeorgeRutherford,AlicenSpaulding
Date: 8Oct2009
Question: ShouldTDFvsABCbeusedforinitialART?(randomizedclinicaltrials)
Settings: Multiplelocations
Bibliography: 1.SaxP,TierneyC,CollierA,FischlM,GodfreyC,JahedN,DrollK,PeeplesL,MyersL,ThalG,RooneyJ,HaB,
WoodwardW,DaarE.ACTG5202:shortertimetovirologicfailure(VF)withabacavir/lamivudine(ABC/3TC)than
tenofovir/emtricitabine(TDF/FTC)aspartofcombinationtherapyintreatment-naïvesubjectswithscreeningHIVRNA
≥100,000c/mL[AbstractTHAB0303].XVIIInternationalConferenceonAIDS,MexicoCity,August3-8,2008.2.Smith
KY,PatelP,FineD,BellosN,SloanL,LackeyP,KumarPN,Sutherland-PhillipsDH,Vavro,C,YauL,WannamakerP,
ShaeferMS,HEATStudyTeam.Randomized,double-blind,placebo-matched,multicentertrialofabacivr/lamivudine
ortenofovir/emtricitabinewithlopinavir/ritonavirforinitialHIVtreatment.AIDS2009;Jul31;23(12):1547-56.
Qualityassessment
Summaryoffindings
Importance
No.ofpatientsEffect
Quality
No.of
stud-
ies
DesignLimitations
Inconsis-
tency
Indirect-
ness
Impreci-
sion
Other
consider-
ations
TDFABC
Relative
(95%CI)
Absolute
Mortality–notreported
0-----None0/0(0%)0/0(0%)--
Clinicalresponse(follow-upmean96weeks)
1Random-
izedtrials
Noserious
limitations
Noserious
inconsis-
tency
Serious1Serious2None3
1/345
(0.3%)
0/343(0%)
RR2.98
(0.12to
72.96)
0moreper
1000(from
0fewerto0
more)
⊕⊕OO
LOW
CRITICAL
Severeadverseevents(follow-upmean96weeks)
1Random-
izedtrials
Noserious
limitations
Noserious
inconsis-
tency
Serious1Noserious
imprecision
None3
97/345
(28.1%)
103/343
(30%)
RR0.94
(0.74to
1.18)
18fewer
per1000
(from78
fewerto54
more)
⊕⊕⊕O
MODER-
ATE
CRITICAL](https://image.slidesharecdn.com/hivguidelinewho2010-120120093817-phpapp02/85/Hiv-guideline-who-2010-106-320.jpg)







![106
Antiretroviral therapy for HIV infection in adults and adolescents
Recommendations for a public health approach
Authors: GeorgeRutherford,AlicenSpaulding
Date: 8Oct2009
Question: ShouldAZTvsd4TbeusedforinitialART?(observationalstudies)
Settings: Multiplesettings
Bibliography: 1.GeorgeC,YesodaA,JayakumarB,LalL.Aprospectivestudyevaluatingclinicaloutcomesandcostsofthree
NNRTI-basedHAARTregimensinKerala,India.JClinPharmTher2009;34:33-40.2.LaurentC,BourgeoisA,Mpoudi-
NgoléE,CiaffiL,KouanfackC,MougnutouR,NkouéN,CalmyA,Koulla-ShiroS,DelaporteE.Tolerabilityand
effectivenessoffirst-lineregimenscombiningnevirapineandlamivudinepluszidovudineorstavudineinCameroon.
AIDSResHumRetroviruses2008;24:393-9.3.MocroftA,PhillipsAN,LedergerberB,KatlamaC,ChiesiA,GoebelFD,
KnyszB,AntunesF,ReissP,LundgrenJD.RelationshipbetweenantiretroviralsusedaspartofacARTregimenand
CD4cellcountincreasesinpatientswithsuppressedviremia.AIDS2006;20:1141-50.4.NjorogeJ,ReidyW,John-
StewartG,AttwaM,KiguruJ,NgumoR,WambuaN,ChungMH.Incidenceofperipheralneuropathyamongpatients
receivingHAARTregimenscontainingstavudinevs.zidovudineinKenya[AbstractTUPEB179].5thConferenceonHIV
PathogenesisandTreatmentandPrevention,CapeTown,SouthAfrica,19−22July2009.5.PazareAR,KhirsagarN,
GogatayN,BajpaiS.Comparativestudyofincidenceofhyperlactetemia/lacticacidosisinstavudinevs.AZTbased
regime[AbstractTHPE0159].XVIIInternationalAIDSConference,MexicoCity,Mexico,3−8August2008.
Qualityassessment
Summaryoffindings
Importance
No.ofpatientsEffect
Quality
No.of
stud-
ies
DesignLimitations
Inconsis-
tency
Indirect-
ness
Impreci-
sion
Other
consider-
ations
AZTd4T
Relative
(95%CI)
Absolute
Mortality(observational)
1Observa-
tional
studies
Noserious
limitations
Noserious
inconsis-
tency
Noserious
indirect-
ness
Noserious
imprecision
None
8/85(9.4%)
11/84
(13.1%)
RR0.72
(0.3to1.7)
37fewer
per1000
(from92
fewerto92
more)
⊕⊕OO
LOW
CRITICAL](https://image.slidesharecdn.com/hivguidelinewho2010-120120093817-phpapp02/85/Hiv-guideline-who-2010-114-320.jpg)




















![128
Antiretroviral therapy for HIV infection in adults and adolescents
Recommendations for a public health approach
27. Gathe J, Jr., Badaro R, Grimwood A, Abrams L, Klesczewski K, Cross A, et al. Antiviral
activity of enteric-coated didanosine, stavudine, and nelfinavir versus zidovudine plus
lamivudine and nelfinavir. J Acquir Immune Defic Syndr 2002;31(4):399-403.
28. Carr A, Chuah J, Hudson J, French M, Hoy J, Law M, et al. A randomised, open-label
comparison of three highly active antiretroviral therapy regimens including two nucleoside
analogues and indinavir for previously untreated HIV-1 infection: the OzCombo1 study.
AIDS 2000;14(9):1171-80.
29. Geijo Martínez MP MMM, Solera Santos J, Barberá Farré JR, Rodríguez Zapata M, Marcos
Sánchez F, Martínez Alfaro E, Cuadra García-Tenorio F, Sanz Moreno J, Moreno Mendaña
JM, Beato Pérez JL, Sanz Sanz J; GECMEI. Ensayo clínico comparativo de eficacia y
seguridad de cuatro pautas de tratamiento antirretroviral de alta eficacia (TARGA) en
pacientes con infección por VIH avanzada [Test comparative clinical efficacy and safety of
four treatment guidelines highly active antiretroviral (TARGA) in patients with advanced
HIV infection]. Rev Clin Esp 2006;206:67-76.
30. Kumar PN, Rodriguez-French A, Thompson MA, Tashima KT, Averitt D, Wannamaker PG,
et al. A prospective, 96-week study of the impact of Trizivir, Combivir/nelfinavir, and
lamivudine/stavudine/nelfinavir on lipids, metabolic parameters and efficacy in
antiretroviral-naive patients: effect of sex and ethnicity. HIV Med 2006;7(2):85-98.
31. Li T, Dai Y, Kuang J, Jiang J, Han Y, Qiu Z, et al. Three generic nevirapine-based antiretroviral
treatments in Chinese HIV/AIDS patients: multicentric observation cohort. PLoS ONE
2008;3(12):e3918.
32. Robbins GK, De Gruttola V, Shafer RW, Smeaton LM, Snyder SW, Pettinelli C, et al.
Comparison of sequential three-drug regimens as initial therapy for HIV-1 infection. N Engl
J Med 2003;349(24):2293-303.
33. Squires KE, Gulick R, Tebas P, Santana J, Mulanovich V, Clark R, et al. A comparison of
stavudine plus lamivudine versus zidovudine plus lamivudine in combination with indinavir
in antiretroviral naive individuals with HIV infection: selection of thymidine analog regimen
therapy (START I). AIDS 2000;14(11):1591-600.
34. The Adult Antiretroviral Treatment and Resistance Study Tshepo [database on the Internet]
2009 [cited November 11, 2009]. Available from: http://clinicaltrials.gov/ct2/show/
NCT00197613?term=Tshepo&rank=1.
35. Gallant JE, Staszewski S, Pozniak AL, DeJesus E, Suleiman JM, Miller MD, et al. Efficacy
and safety of tenofovir DF vs stavudine in combination therapy in antiretroviral-naive
patients: a 3-year randomized trial. JAMA 2004;292(2):191-201.
36. Rey D, Hoen B, Chavanet P, Schmitt MP, Hoizey G, Meyer P, et al. High rate of early
virological failure with the once-daily tenofovir/lamivudine/nevirapine combination in naive
HIV-1-infected patients. J Antimicrob Chemother 2009;63(2):380-8.](https://image.slidesharecdn.com/hivguidelinewho2010-120120093817-phpapp02/85/Hiv-guideline-who-2010-136-320.jpg)

![130
Antiretroviral therapy for HIV infection in adults and adolescents
Recommendations for a public health approach
48. Fernandez Lison LC. PDLLE, Hevia Alonso A, Garrido Martinez MT, Bocanegra Martin C.
Cost-effectiveness analysis of tenofovir versus zidovudine in combination therapy with
efavirenz and lamivudine for the treatment of HIV in naive patients. Farmacia Hospitalaria
2005(29):11-7.
49. Ayala Gaytan JJ dlGE, Garcia MC, Chavez SBV. Nevirapine or efavirenz in combination
with two nucleoside analogues in HIV infected antiretroviral naïve patients. Med Intern Mex
2004;20:24.
50. Manosuthi W, Sungkanuparph S, Tantanathip P, Lueangniyomkul A, Mankatitham W,
Prasithsirskul W, et al. A randomized trial comparing plasma drug concentrations and
efficacies between 2 nonnucleoside reverse-transcriptase inhibitor-based regimens in
HIV-infected patients receiving rifampicin: the N2R Study. Clin Infect Dis 2009;48(12):1752-
9.
51. Nuñez M, Soriano V, Martin-Carbonero L, Barrios A, Barreiro P, Blanco F, et al. SENC
(Spanish efavirenz vs. nevirapine comparison) trial: a randomized, open-label study in
HIV-infected naive individuals. HIV clinical trials 2002;3(3):186-94.
52. Sow PG BM, Diallo PD, Lo I, Ndiaye B, Gaye AM, editor. Efficacy and safety of
lamivudine+zidovudine+efavirenz and lamivudine+zidovudine+névirapine in treatment
HIV1 infected patients. A retrospective cross study analysis. XVI International AIDS
Conference; 13-18 August 2006: Toronto, Canada.
53. van den Berg-Wolf M, Hullsiek KH, Peng G, Kozal MJ, Novak RM, Chen L, et al. Virologic,
immunologic, clinical, safety, and resistance outcomes from a long-term comparison of
efavirenz-based versus nevirapine-based antiretroviral regimens as initial therapy in HIV-
1-infected persons. HIV clinical trials 2008;9(5):324-36.
54. van Leth F, Phanuphak P, Ruxrungtham K, Baraldi E, Miller S, Gazzard B, et al. Comparison
of first-line antiretroviral therapy with regimens including nevirapine, efavirenz, or both
drugs, plus stavudine and lamivudine: a randomised open-label trial, the 2NN Study.
Lancet 2004;363(9417):1253-63.
55. Clinicaltrials.gov. Comparison of nevirapine and efavirenz for the treatment of HIV-TB
coInfected patients (ANRS 12146 CARINEMO). 2009; Available from: http://clinicaltrials.
gov/ct2/show/NCT00495326?term=ANRS+12146&rank=1.
56. Evaluation of 4 new simplified antiretroviral treatments in naive HIV-1 infected patients in
Africa (ANRS 12115 DAYANA) [database on the Internet] 2009. Available from: http://
clinicaltrials.gov/ct2/show/NCT00573001?term=DAYANA&rank=1.
57. Rajesh L, Karunaianantham R, Narayanan PR, Swaminathan S. Antiretroviral drug-resistant
mutations at baseline and at time of failure of antiretroviral therapy in HIV type 1-coinfected
TB patients. AIDS Res Hum Retroviruses 2009;25(11):1179-85.
58. Gilead Sciences. Viread prescribing information. 2010 (Revised 03/2010 ).](https://image.slidesharecdn.com/hivguidelinewho2010-120120093817-phpapp02/85/Hiv-guideline-who-2010-138-320.jpg)


![133
83. Baylor MS, Johann-Liang R. Hepatotoxicity associated with nevirapine use. J Acquir
Immune Defic Syndr 2004;35(5):538-9.
84. Feinberg J. Report from the 16th Conference on Retroviruses and Opportunistic Infections.
Lopinavir/r is superior to nevirapine in women who previously received single-dose
nevirapine. AIDS Clin Care 2009;21(4):33.
85. Sax PE, Gallant JE, Klotman PE. Renal safety of tenofovir disoproxil fumarate. AIDS Read
2007;17(2):90-2,9-104,C3.
86. Roling J, Schmid H, Fischereder M, Draenert R, Goebel FD. HIV-associated renal diseases
and highly active antiretroviral therapy-induced nephropathy. Clin Infect Dis
2006;42(10):1488-95.
87. Cassetti I, Madruga JV, Suleiman JM, Etzel A, Zhong L, Cheng AK, et al. The safety and
efficacy of tenofovir DF in combination with lamivudine and efavirenz through 6 years in
antiretroviral-naive HIV-1-infected patients. HIV clinical trials 2007;8(3):164-72.
88. Nurutdinova D, Onen NF, Hayes E, Mondy K, Overton ET. Adverse effects of tenofovir use
in HIV-infected pregnant women and their infants. Ann Pharmacother 2008;42(11):1581-5.
89. WHO, UNAIDS and UNICEF. Towards universal access: Scaling up of priority HIV/AIDS
interventions in the health sector: Progress report 2009 [cited 2009 Nov 11, 2009]:
Available from: http://www.who.int/hiv/pub/2009progressreport/en/.
90. Gallant JE, DeJesus E, Arribas JR, Pozniak AL, Gazzard B, Campo RE, et al. Tenofovir DF,
emtricitabine, and efavirenz vs. zidovudine, lamivudine, and efavirenz for HIV. N Engl J
Med 2006;354(3):251-60.
91. Subbaraman R, Chaguturu SK, Mayer KH, Flanigan TP, Kumarasamy N. Adverse effects of
highly active antiretroviral therapy in developing countries. Clin Infect Dis 2007;45(8):1093-
101.
92. McComsey G, Lonergan JT. Mitochondrial dysfunction: patient monitoring and toxicity
management. J Acquir Immune Defic Syndr 2004;37 Suppl 1:S30-5.
93. Hawkins C, Achenbach C, Fryda W, Ngare D, Murphy R. Antiretroviral durability and
tolerability in HIV-infected adults living in urban Kenya. J Acquir Immune Defic Syndr
2007;45(3):304-10.
94. van Griensven J, Zachariah R, Rasschaert F, Mugabo J, Atte EF, Reid T. Stavudine- and
nevirapine-related drug toxicity while on generic fixed-dose antiretroviral treatment:
incidence, timing and risk factors in a three-year cohort in Kigali, Rwanda. Trans R Soc
Trop Med Hyg 2010; 104(2): 148-53.
95. Kallianpur AR, Hulgan T. Pharmacogenetics of nucleoside reverse-transcriptase inhibitor-
associated peripheral neuropathy. Pharmacogenomics 2009;10(4):623-37.](https://image.slidesharecdn.com/hivguidelinewho2010-120120093817-phpapp02/85/Hiv-guideline-who-2010-141-320.jpg)
![134
Antiretroviral therapy for HIV infection in adults and adolescents
Recommendations for a public health approach
96. van Griensven J, De Naeyer L, Mushi T, Ubarijoro S, Gashumba D, Gazille C, et al. High
prevalence of lipoatrophy among patients on stavudine-containing first-line antiretroviral
therapy regimens in Rwanda. Trans R Soc Trop Med Hyg 2007;101(8):793-8.
97. Mutimura E, Stewart A, Rheeder P, Crowther NJ. Metabolic function and the prevalence of
lipodystrophy in a population of HIV-infected African subjects receiving highly active
antiretroviral therapy. J Acquir Immune Defic Syndr 2007;46(4):451-5.
98. Geddes R, Knight S, Moosa MY, Reddi A, Uebel K, Sunpath H. A high incidence of
nucleoside reverse transcriptase inhibitor (NRTI)-induced lactic acidosis in HIV-infected
patients in a South African context. S Afr Med J 2006;96(8):722-4.
99. WHO. Antiretroviral therapy for HIV infection in adults and adolescents:Recommendations
for a public health approach. 2006. Available from: http://www.who.int/hiv/pub/guidelines/
artadultguidelines.pdf.
100. Tai JH, Udoji MA, Barkanic G, Byrne DW, Rebeiro PF, Byram BR, et al. Pregnancy and HIV
disease progression during the era of highly active antiretroviral therapy. J Infect Dis
2007;196(7):1044-52.
101. The antiretroviral pregnancy registry [database on the Internet]. Antiretroviral Pregnancy
Registry Steering Committee. 2009. Available from: http://www.apregistry.com/forms/
interim_report.pdf.
102. Peltier CA, Ndayisaba GF, Lepage P, van Griensven J, Leroy V, Pharm CO, et al.
Breastfeeding with maternal antiretroviral therapy or formula feeding to prevent HIV
postnatal mother-to-child transmission in Rwanda. AIDS 2009;23(18):2415-23.
103. Ouyang DW, Shapiro DE, Lu M, Brogly SB, French AL, Leighty RM, et al. Increased risk of
hepatotoxicity in HIV-infected pregnant women receiving antiretroviral therapy independent
of nevirapine exposure. AIDS 2009;23(18):2425-30.
104. Musoke P, Guay LA, Bagenda D, Mirochnick M, Nakabiito C, Fleming T, et al. A phase I/II
study of the safety and pharmacokinetics of nevirapine in HIV-1-infected pregnant
Ugandan women and their neonates (HIVNET 006). AIDS 1999;13(4):479-86.
105. Kunz A, Frank M, Mugenyi K, Kabasinguzi R, Weidenhammer A, Kurowski M, et al.
Persistence of nevirapine in breast milk and plasma of mothers and their children after
single-dose administration. J Antimicrob Chemother 2009;63(1):170-7.
106. Muro E, Droste JA, Hofstede HT, Bosch M, Dolmans W, Burger DM. Nevirapine plasma
concentrations are still detectable after more than 2 weeks in the majority of women
receiving single-dose nevirapine: implications for intervention studies. J Acquir Immune
Defic Syndr 2005;39(4):419-21.
107. Ribaudo HJ, Haas DW, Tierney C, Kim RB, Wilkinson GR, Gulick RM, et al. Pharmacogenetics
of plasma efavirenz exposure after treatment discontinuation: an Adult AIDS Clinical Trials
Group Study. Clin Infect Dis 2006;42(3):401-7.](https://image.slidesharecdn.com/hivguidelinewho2010-120120093817-phpapp02/85/Hiv-guideline-who-2010-142-320.jpg)





![140
Antiretroviral therapy for HIV infection in adults and adolescents
Recommendations for a public health approach
166. S Lang M-KM, Cotte L. Impact of specific NRTI and PI exposure on the risk of myocardial
infarction: A case-control study nested within FHDH ANRSC04. 16th Conference on
Retroviruses and Opportunistic Infections; Montreal, Canada. 2009.
167. Arribas JR, Pulido F, Delgado R, Lorenzo A, Miralles P, Arranz A, et al. Lopinavir/ritonavir
as single-drug therapy for maintenance of HIV-1 viral suppression: 48-week results of a
randomized, controlled, open-label, proof-of-concept pilot clinical trial (OK Study). J
Acquir Immune Defic Syndr 2005;40(3):280-7.
168. Escobar I, Pulido F, Perez E, Arribas JR, Garcia MP, Hernando A. [Pharmacoeconomic
analysis of a maintenance strategy with lopinavir/ritonavir monotherapy in HIV-infected
patients]. Enferm Infecc Microbiol Clin 2006;24(8):490-4.
169. Cameron DW, da Silva Barbara A, Arribas Jose R, Myers Robert A, Bellos Nicholaos C,
Gilmore N, et al. A 96/Week Comparison of Lopinavir/Ritonavir Combination Therapy
Followed by Lopinavir/Ritonavir Monotherapy versus Efavirenz Combination Therapy. J
Infect Dis 2008;198(2):234-40.
170. Arribas J. JG, G. Fatkenheuer, M. Nelson, N. Clumeck, F. Pulido et al. The MONET trial:
darunavir/ritonavir monotherapy shows non-inferior efficacy to standard HAART, for patients
with HIV RNA < 50 copies/mL at baseline. 5th IAS Conference on HIV Pathogenesis,
Treatment and Prevention; Cape Town. 2009.
171. C Katlama VM, Algarte-Genin M, Duvivier C, Lambert-Niclot S, Girard PM et al. Efficacy of
darunavir/ritonavir as single-drug maintenance therapy in patients with HIV-1 viral
suppression: a randomized open-label non-inferiority trial, MONOI-ANRS 136. 5th IAS
Conference on HIV Pathogenesis, Treatment and Prevention; Cape Town.
172. Delfraissy JF, Flandre P, Delaugerre C, Ghosn J, Horban A, Girard PM, et al. Lopinavir/
ritonavir monotherapy or plus zidovudine and lamivudine in antiretroviral-naive HIV-
infected patients. AIDS 2008;22(3):385-93.
173. Bierman WF, van Agtmael MA, Nijhuis M, Danner SA, Boucher CA. HIV monotherapy with
ritonavir-boosted protease inhibitors: a systematic review. AIDS 2009;23(3):279-91.
174. Elliott JH, Lynen L, Calmy A, De Luca A, Shafer RW, Zolfo M, et al. Rational use of
antiretroviral therapy in low-income and middle-income countries: optimizing regimen
sequencing and switching. AIDS 2008;22(16):2053-67.
175. Evaluation of three strategies of second-line antiretroviral treatment in Africa (Dakar –
Bobo-Dioulasso – Yaoundé) (2LADY) [database on the Internet] 2009. Available from:
http://clinicaltrials.gov/ct2/show/NCT00928187?term=2LADY&rank=1.
176. Murphy R Sunpath H, Nijhawan A, McLellan M , Kuritzkes D. Lopinavir/ritonavir (LPV/r) + 2
nucleoside analogues as second-line ART in Protease-inhibitor naïve adults in South Africa:
Outcomes and adverse effects. 15th Conference on Retroviruses and Opportunistic
Infections; 3-6 February 2008; Boston, USA..](https://image.slidesharecdn.com/hivguidelinewho2010-120120093817-phpapp02/85/Hiv-guideline-who-2010-148-320.jpg)


![143
201. Walker AS, Ford D, Gilks CF, Munderi P, Ssali F, Reid A, et al. Daily co-trimoxazole
prophylaxis in severely immunosuppressed HIV-infected adults in Africa started on
combination antiretroviral therapy: an observational analysis of the DART cohort. Lancet
2010;375(9722):1278-86.
202. Mitchell SK, Kelly KJ, Potgieter FE, Moon MW. Assessing social preparedness for
antiretroviral therapy in a generalized AIDS epidemic: a diffusion of innovations approach.
AIDS Behav 2009;13(1):76-84.
203. Orrell C. Antiretroviral adherence in a resource-poor setting. Curr HIV/AIDS Rep
2005;2(4):171-6.
204. Sodergard B, Hofer S, Halvarsson M, Sonnerborg A, Tully MP, Lindblad AK. A structural
equation modeling approach to the concepts of adherence and readiness in antiretroviral
treatment. Patient Educ Couns 2007;67(1-2):108-16.
205. Tabarsi P, Saber-Tehrani AS, Baghaei P, Padyab M, Mansouri D, Amiri M, et al. Early
initiation of antiretroviral therapy results in decreased morbidity and mortality among
patients with TB and HIV. J Int AIDS Soc 2009;12(1):14.
206. Zolopa A, Andersen J, Powderly W, Sanchez A, Sanne I, Suckow C, et al. Early antiretroviral
therapy reduces AIDS progression/death in individuals with acute opportunistic infections:
a multicenter randomized strategy trial. PLoS ONE 2009;4(5):e5575.
207. Lawn SD, Harries AD, Wood R. Strategies to reduce early morbidity and mortality in adults
receiving antiretroviral therapy in resource-limited settings. Curr Opin HIV AIDS
2010;5(1):18-26.
208. WHO. Towards universal access. Scaling up priority HIV/AIDS interventions in the health
sector. 2009 Progress Report. 2009.
209. Gray RH, Wawer MJ, Brookmeyer R, Sewankambo NK, Serwadda D, Wabwire-Mangen F,
et al. Probability of HIV-1 transmission per coital act in monogamous, heterosexual, HIV-1-
discordant couples in Rakai, Uganda. Lancet 2001;357(9263):1149-53.
210. Pao D, Pillay D, Fisher M. Potential impact of early antiretroviral therapy on transmission.
Curr Opin HIV AIDS 2009;4(3):215-21.
211. DART Trial Team. Routine versus clinically driven laboratory monitoring of HIV antiretroviral
therapy in Africa (DART): a randomised non-inferiority trial. Lancet 2010;375(9709):123-31.
212. Braitstein P, Brinkhof MW, Dabis F, Schechter M, Boulle A, Miotti P, et al. Mortality of HIV-
1-infected patients in the first year of antiretroviral therapy: comparison between low-
income and high-income countries. Lancet 2006;367(9513):817-24.
213. Effectiveness of HIV viral load monitoring of patient outcome in resource-poor settings
[database on the Internet]2009 [cited Februrary 28, 2010]. Available from: http://
clinicaltrials.gov/ct2/show/NCT00929604?term=Saag&cntry1=AF:ZM&rank=1.](https://image.slidesharecdn.com/hivguidelinewho2010-120120093817-phpapp02/85/Hiv-guideline-who-2010-151-320.jpg)
![144
Antiretroviral therapy for HIV infection in adults and adolescents
Recommendations for a public health approach
214. Monitoring highly active antiretroviral therapy in HIV-infected parentsin Thailand [database
on the Internet] 2009 Last Updated: September 14 [cited Frebbrury 18, 2010]. Available
from: http://clinicaltrials.gov/ct2/show/NCT00162682?term=Lallemant&cntry1=SE:TH&ra
nk=4.
215. Antiretroviral treatment simplified follow-up management assessment (ANRS 12110
STRATALL) [database on the Internet] 2008 Last updated: April 16, 2008. Available from:
http://clinicaltrials.gov/ct2/show/NCT00301561?term=Laurent&cntry1=AF:CM&rank=1.
216. Goicoechea M, Liu S, Best B, Sun S, Jain S, Kemper C, et al. Greater tenofovir-associated
renal function decline with protease inhibitor-based versus nonnucleoside reverse-
transcriptase inhibitor-based therapy. J Infect Dis 2008;197(1):102-8.
217. Mohsen AH, Easterbrook PJ, Taylor C, Portmann B, Kulasegaram R, Murad S, et al. Impact
of human immunodeficiency virus (HIV) infection on the progression of liver fibrosis in
hepatitis C virus infected patients. Gut 2003;52(7):1035-40.
218. Smit C, van den Berg C, Geskus R, Berkhout B, Coutinho R, Prins M. Risk of hepatitis-
related mortality increased among hepatitis C virus/HIV-coinfected drug users compared
with drug users infected only with hepatitis C virus: a 20-year prospective study. J Acquir
Immune Defic Syndr 2008;47(2):221-5.
219. Benhamou Y, Bochet M, Di Martino V, Charlotte F, Azria F, Coutellier A, et al. Liver fibrosis
progression in human immunodeficiency virus and hepatitis C virus coinfected patients.
The Multivirc Group. Hepatology 1999;30(4):1054-8.
220. Chen TY, Ding EL, Seage Iii GR, Kim AY. Meta-analysis: increased mortality associated
with hepatitis C in HIV-infected persons is unrelated to HIV disease progression. Clin Infect
Dis 2009;49(10):1605-15.
221. Mocroft A, Rockstroh J, Soriano V, Ledergerber B, Kirk O, Vinogradova E, et al. Are specific
antiretrovirals associated with an increased risk of discontinuation due to toxicities or
patient/physician choice in patients with hepatitis C virus coinfection? Antivir Ther
2005;10(7):779-90.
222. Roche. Copegus (ribavirin, USP) prescibing information. 2010.
223. Bani-Sadr F, Denoeud L, Morand P, Lunel-Fabiani F, Pol S, Cacoub P, et al. Early virologic
failure in HIV-coinfected hepatitis C patients treated with the peginterferon-ribavirin
combination: does abacavir play a role? J Acquir Immune Defic Syndr 2007;45(1):123-5.
224. Rodriguez-Torres M, Torriani FJ, Soriano V, Borucki MJ, Lissen E, Sulkowski M, et al. Effect
of ribavirin on intracellular and plasma pharmacokinetics of nucleoside reverse
transcriptase inhibitors in patients with human immunodeficiency virus-hepatitis C virus
coinfection: results of a randomized clinical study. Antimicrob Agents Chemother
2005;49(10):3997-4008.](https://image.slidesharecdn.com/hivguidelinewho2010-120120093817-phpapp02/85/Hiv-guideline-who-2010-152-320.jpg)




Hiv guideline who 2010
- 1. Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach 2010revision AntiretroviraltherapyforHIVinfectioninadultsandadolescentsRecommendationsforapublichealthapproach2010revision Strengthening health services to fight HIV/AIDS HIV/AIDS ProgrammeFor more information, contact: World Health Organization Department of HIV/AIDS 20, avenue Appia 1211 Geneva 27 Switzerland E-mail: [email protected] www.who.int/hiv ISBN 978 92 4 159976 4
- 2. WHO Library Cataloguing-in-Publication Data Antiretroviral therapy for HIV infection in adults and adolescents: recommendations for a public health approach. – 2010 rev. 1.Anti-retroviral agents - therapeutic use. 2.Anti-retroviral agents - pharmacology. 3.HIV infections – drug therapy. 4.Adult. 5.Adolescent. 6.Guidelines. 7.Developing countries. I.World Health Organization. ISBN 978 92 4 159976 4 (NLM classification: WC 503.2) © World Health Organization 2010 All rights reserved. Publications of the World Health Organization can be obtained from WHO Press, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel.: +41 22 791 3264; fax: +41 22 791 4857; e-mail: [email protected]). Requests for permission to reproduce or translate WHO publications – whether for sale or for noncommercial distribution – should be addressed to WHO Press, at the above address (fax: +41 22 791 4806; e-mail: [email protected]). The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement. The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters. All reasonable precautions have been taken by the World Health Organization to verify the information contained in this publication. However, the published material is being distributed without warranty of any kind, either expressed or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall the World Health Organization be liable for damages arising from its use. Printed in Austria
- 3. Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach 2010 revision
- 5. iii 1. Acronyms and abbreviations............................................................................................... 1 2. Acknowledgements............................................................................................................. 5 3. Executive summary............................................................................................................. 7 4. Background......................................................................................................................... 8 5. Funding and declarations of interest................................................................................... 9 6. Guiding principles............................................................................................................. 10 7. Objectives of the guidelines and target audience..............................................................11 8. Methodology and process................................................................................................ 12 9. From evidence to recommendation.................................................................................. 14 10. Adapting the guidelines.................................................................................................... 17 11. Summary of changes........................................................................................................ 19 12. Recommendations at a glance......................................................................................... 20 13. When to start..................................................................................................................... 24 13.1. Recommendations................................................................................................ 24 13.2. Evidence................................................................................................................ 24 13.3. Summary of findings.............................................................................................. 25 13.4. Benefits and risks.................................................................................................. 26 13.5. Acceptability and feasibility................................................................................... 26 13.6. Clinical considerations.......................................................................................... 27 14. What to start...................................................................................................................... 31 14.1. Recommendations................................................................................................ 31 14.2. Evidence................................................................................................................ 31 14.3. Summary of main findings..................................................................................... 32 14.4. Benefits and risks.................................................................................................. 33 14.5. Acceptability and feasibility................................................................................... 33 14.6. The choice between NVP and EFV........................................................................ 34 14.7. AZT + 3TC + EFV option...................................................................................... 35 14.8. AZT + 3TC + NVP option...................................................................................... 36 14.9. TDF + 3TC (or FTC) + EFV option........................................................................ 37 14.10. TDF + 3TC (or FTC) + NVP option........................................................................ 38 14.11. Triple NRTI option.................................................................................................. 39 14.12. Stavudine (d4T)..................................................................................................... 39 14.13. NRTIs not to be used together............................................................................... 40 Contents
- 6. iv Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach 15. Specific populations – when and what to start................................................................. 41 15.1. Recommendations for HIV-infected pregnant women........................................... 41 15.2. Recommendations for women with prior exposure to antiretrovirals for PMTCT... 42 15.3. Recommendations for HIV/HBV coinfection.......................................................... 44 15.4. Recommendations for HIV/tuberculosis coinfection............................................. 45 15.5. Rifabutin................................................................................................................ 46 16. When to switch ART.......................................................................................................... 48 16.1. Recommendations................................................................................................ 48 16.2. Evidence................................................................................................................ 48 16.3. Summary of findings.............................................................................................. 48 16.4. Benefits and risks.................................................................................................. 49 16.5. Clinical considerations.......................................................................................... 50 17. Second-line regimens....................................................................................................... 53 17.1. Recommendations.................................................................................................... 53 17.2. Evidence................................................................................................................ 53 17.3. Summary of findings.............................................................................................. 53 17.4. Benefits and risks.................................................................................................. 54 17.5. Acceptability and feasibility................................................................................... 54 17.6. Clinical considerations.......................................................................................... 55 17.7. Selection of second-line NRTIs............................................................................. 56 17.8. Maintaining 3TC in the second-line regimen......................................................... 56 17.9. NRTIs for HIV/HBV coinfection.............................................................................. 57 17.10. Selection of boosted protease inhibitor................................................................. 57 18. Third-line regimens........................................................................................................... 58 18.1. Recommendations.................................................................................................... 58 18.2. Evidence................................................................................................................ 58 18.3. Summary of findings.............................................................................................. 58 18.4. Benefits and risks.................................................................................................. 59 18.5. Acceptability and feasibility................................................................................... 59 18.6. Clinical considerations.......................................................................................... 60 19. Package of care interventions........................................................................................... 61 19.1. Guiding principles................................................................................................. 61 19.2. Voluntary counselling and testing and provider-initiated testing and counselling..... 61 19.3. Preventing further transmission of HIV.................................................................. 61 19.4. The Three I's for HIV/TB......................................................................................... 62 19.5. Cotrimoxazole prophylaxis.................................................................................... 62 19.6. Sexually transmitted infections.............................................................................. 62 19.7. Treatment preparedness....................................................................................... 63 19.8. Early initiation of ART............................................................................................. 63 19.9. ART as prevention................................................................................................. 63
- 7. v 20. Laboratory monitoring....................................................................................................... 64 20.1. Guiding principles................................................................................................. 64 20.2. Laboratory monitoring on ART.............................................................................. 65 21. Annexes............................................................................................................................. 67 21.1. Special note on coinfection with HIV and hepatitis C............................................ 67 21.2. Dosages of recommended antiretrovirals............................................................. 67 21.3. Toxicities and recommended drug substitutions................................................... 69 21.4. ARV-related adverse events and recommendations............................................. 71 21.5. Diagnostic criteria for HIV-related clinical events.................................................. 73 21.6. Grading of selected clinical and laboratory toxicities............................................ 81 21.7. Prevention and assessment of HIV drug resistance.............................................. 86 21.8. Special note on antiretroviral pharmacovigilance.................................................. 87 21.9. GRADE evidence tables........................................................................................ 89 22. References...................................................................................................................... 126
- 9. 1 3TC lamivudine AB antibody ABC abacavir ACTG AIDS Clinical Trials Group AIDS acquired immunodeficiency syndrome ALT alanine aminotransferase ANC antenatal clinic ART antiretroviral therapy ARV antiretroviral AST aspartate aminotransferase ATV atazanavir AZT zidovudine (also known as ZDV) BID twice daily BMI body mass index bPI boosted protease inhibitor CD4 cell T-lymphocyte bearing CD4 receptor CEM cohort event monitoring CMV cytomegalovirus CNS central nervous system CXR chest X-ray d4T stavudine DART Development of Antiretroviral Therapy (in Africa) DBS dried blood spot ddI didanosine DNA deoxyribonucleic acid DRV darunavir EC enteric-coated EFV efavirenz EIA enzyme immunoassay ETV etravirine EPTB extrapulmonary tuberculosis FBC full blood count FDC fixed-dose combination FPV fos-amprenavir FTC emtricitabine 1. Acronyms and abbreviations
- 10. 2 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach GDG Guidelines Development Group GI gastrointestinal GNP+ Global Network of People Living with HIV GRADE Grading of Recommendations Assessment, Development and Evaluation Hb haemoglobin HBV hepatitis B virus HCV hepatitis C virus HDL high-density lipoprotein HIV human immunodeficiency virus HIVDR HIV drug resistance HIVRNA human immunodeficiency virus ribonucleic acid HSV herpes simplex virus ICW International Community of Women Living with HIV/AIDS IDU injecting drug user IDV indinavir INH isoniazid IRIS immune reconstitution inflammatory syndrome ITCP International Treatment Preparedness coalition LPV lopinavir LPV/r lopinavir/ritonavir MTCT mother-to-child transmission (of HIV) NAM nucleoside/nucleotide analogue mutation NFV nelfinavir NNRTI non-nucleoside reverse transcriptase inhibitor NRTI nucleoside reverse transcriptase inhibitor NVP nevirapine OBR optimized background regimen OI opportunistic infection OST opioid substitution treatment PCP Pneumocystis jiroveci pneumonia PEPFAR President’s Emergency Plan for AIDS Relief PETRA Perinatal Transmission Study PGL persistent generalized lymphadenopathy PI protease inhibitor PLHIV people living with HIV
- 11. 3 PML progressive multifocal leukoencephalopathy PMTCT prevention of mother-to-child transmission (of HIV) /r low-dose ritonavir RAL raltegravir RBV ribavirin RCT randomized clinical trial RNA ribonucleic acid RT reverse transcriptase RTI reverse transcriptase inhibitor RTV ritonavir Sd-NVP single-dose nevirapine SJS Stevens-Johnson syndrome SQV saquinavir STI structured treatment interruption TB tuberculosis TDF tenofovir disoproxil fumarate TEN toxic epidermal necrolysis TLC total lymphocyte count VL viral load ULN upper limit of normal UNAIDS Joint United Nations Programme on HIV/AIDS WBC white blood cell count WHO World Health Organization
- 13. 5 The World Health Organization wishes to express its gratitude to the following institutions, technical committees and consultants for their contributions to the revision of the antiretroviral treatment recommendations for HIV-infected adults and adolescents. University of California, San Francisco, USA Jamal Harris, Tara Horvath, Eliza Humphreys, Gail Kennedy, George Rutherford, Karen Schlein, Sarah Wan, Gavrilah Wells, Rose Whitmore South African Cochrane Centre, Medical Research Council of South Africa, Cape Town, South Africa Joy Oliver, Elizabeth Pienaar, Nandi Siegfried University of California, Berkeley, USA Andrew Anglemyer University of Minnesota, USA Alicen Spaulding Johns Hopkins University, USA Larry Chang University of North Carolina, USA Amitabh Suthar University of Birmingham, UK Olalekan Uthman McMaster University, Canada Nancy Santesso, Holger Schünemann, University of Alberta, Canada Ameeta Singh, Thomas Wong University of Liverpool, UK David Back, Sara Gibbons, Saye Khoo, Kay Seden Griffith University, Australia Patricia Whyte University of Bern, Switzerland Martin Brinkhof, Mathias Egger, Olivia Keiser Global Network of People Living with HIV/AIDS (GNP+) International Community of Women Living with HIV/AIDS Southern Africa (ICW) Members of the WHO ART Guidelines Committee Carlos Avila (UNAIDS, Switzerland), Lori Bollinger (Futures Institute, USA), Alexandra Calmy (University of Geneva, Switzerland), Zengani Chirwa (Ministry of Health, Malawi), Francois Dabis (ISPED, France), Shaffiq Essajee (Clinton Foundation, USA), Loon Gangte (GNP+, India), Julian Gold (University of New South Wales, Australia), James Hakim (University of Zimbabwe, 2. Acknowledgements
- 14. 6 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach Zimbabwe), Charles Holmes (PEPFAR, USA), Robert Josiah (NACP, Tanzania), Ayesha Khan (Ministry of Health, Pakistan), Stephen Lawn (University of Cape Town, South Africa), Frank Lule (WHO AFRO, Congo), Jean-Paul Moatti (INSERM, France), Lynne Mofenson (NIH, USA), Irene Mukui (Ministry of Public Health and Sanitation, Kenya), Paula Munderi (Uganda Virus Research Institute, Uganda), Mutinta Nalubamba (Ministry of Health, Zambia), Portia Ngcaba (TAC, South Africa), Megan O’Brien (Clinton Foundation, USA), Sylvia Ojoo (Institute of Human Virology, Kenya), Vladimir Osin (ITPC, Russia), Praphan Phanuphak (Thai Red Cross, Thailand), BB Rewari (National AIDS Control Organization, India), Papa Salif Sow (University of Dakar, Senegal), Omar Sued (WHO AMRO, USA), Tengiz Tsertsvadze (National AIDS Programme, Georgia), Rochelle Walensky (Harvard Center for AIDS Research, USA), Robin Wood (University of Cape Town, South Africa), Augustin Yuma (National HIV/AIDS Programme, Democratic Republic of Congo), Oleg Yurin (Central Institute of Epidemiology, Russia). External peer reviewers Xavier Anglaret (University of Bordeaux, France), Stefano Lazzari (Global Fund for AIDS, Tuberculosis and Malaria, Switzerland), Veronique Bortolotti (WHO EMRO, Egypt), Pedro Cahn (Fundación Huesped, Argentina), Serge Eholie (ANEPA, Côte d'Ivoire), Jean Baptiste Guiard- Schmid (WHO AFRO, Burkina Faso), Scott Hammer (Columbia University, USA), Mark Harrington (TAG, USA), Elly Katabira (Makerere University, Uganda), Ricardo Kuchembecker (Ministry of Health, Brazil), Nagalingeswaran Kumarasamy (YRG Care, India), Barbara Marston (CDC, USA), Elliot Raizes (CDC, USA), Padmini Srikantiah (WHO SEARO, India). WHO also wishes to acknowledge comments and contributions made by Jacqueline Bataringaya (International AIDS Society, Switzerland), Silvia Bertagnolio (WHO/HTM/HIV), Jose Maria Garcia Calleja (WHO/HTM/HIV), Helen Chun (Department of Defense, USA), Suzanne Crowe (Burnet Institute, Australia), Micheline Diepart (WHO/HTM/HIV), Boniface Dongmo (WHO/HTM/HIV), Andrew Doupe (WHO/HTM/HIV), Ted Ellenbrook (CDC, USA), Robert Ferris (PEPFAR, USA), Haileyesus Getahun (WHO/HTM/STB), Sarah Glover (LSHTM, United Kingdom), Reuben Granich (WHO/HTM/HIV), Catherine Godfrey (NIH, USA), Alexandre Hamilton (St. Vincent's Hospital, Australia), John Kaplan (CDC, USA), John Liddy (independent consultant, Thailand), Mary Lou Ludgren (CDC, USA), Brian McMahon (CDC, USA), Thomas Minior (PEPFAR, USA), Neil Parkin (WHO/HTM/HIV), Francoise Renaud-Thery (WHO/HIV/SIR), Erik Schouten (Ministry of Health, Malawi), Delphine Sculier (WHO/HTM/STB), Nathan Shaffer (WHO/HTM/HIV), Tin Tin Sint (WHO/ HTM/HIV), Yves Souteyrand (WHO/HTM/HIV), Steven Wiersma (WHO/FCH/IVB) and Paul Weidle (CDC, USA). Special thanks go to Victoria Anagbo, Sally Girvin and Nadia Hilal of WHO/HTM/HIV, who provided administrative support, and to Chris Duncombe of HIVNAT Research Network (Thailand) and the University of New South Wales (Australia), who was the major writer of the ART guidelines document. The work was coordinated by Siobhan Crowley and Marco Vitoria of WHO/HTM/HIV, Geneva, Switzerland.
- 15. 7 Since the publication in 2006 of Antiretroviral therapy for HIV infection in adults and adolescents: Recommendations for a public health approach, new evidence has emerged on when to initiate ART, optimal ART regimens, the management of HIV coinfection with tuberculosis and chronic viral hepatitis and the management of ART failure. This evidence formed the basis for the recommendations contained in the 2010 update, which outlines a public health approach to the delivery of ART for adults and adolescents in settings with limited health systems capacity and resources. The recommendations were based on the preparation GRADE evidence profiles, systematic and targeted reviews, risk-benefit analyses, consultations with PLHIV, technical reports, and assessments of impact, feasibility and cost. This guideline revision was conducted in accordance with procedures outlined by the WHO Guidelines Review Committee and is based on the GRADE approach to evidence review. The process involved four separate working groups: the Internal WHO ART Guideline Working Group, the ART Guideline Drafting Group, the external ART Peer Review Panel and the full ART Guideline Review Committee. The consensus recommendations, which emerged from consultations of the working groups, encourage earlier HIV diagnosis and earlier antiretroviral treatment, and promote the use of less toxic regimens and more strategic laboratory monitoring. The guidelines identify the most potent, effective and feasible first-line, second-line and subsequent treatment regimens, applicable to the majority of populations, the optimal timing of ART initiation and improved criteria for ART switching, and introduce the concept of third-line antiretroviral regimens. The primary audiences are national treatment advisory boards, partners implementing HIV care and treatment, and organizations providing technical and financial support to HIV care and treatment programmes in resource-limited settings. It is critical that national ART programme and public health leaders consider these recommendations in the context of countries’ HIV epidemics, the strengths and weaknesses of health systems, and the availability of financial, human and other essential resources. In adapting these guidelines, care must be exercised to avoid undermining current treatment programmes, to protect access for the most at-risk populations, to achieve the greatest impact for the greatest number of people and to ensure sustainability. It is similarly important to ensure that the adaptation of these guidelines do not stifle ongoing or planned research, since the new recommendations reflect the current state of knowledge and new information for sustainability and future modifications of existing guidelines will be needed. 3. Executive summary
- 16. 8 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach WHO guidelines for ART for HIV infection in adults and adolescents were originally published in 2002, and were revised in 2003 and 2006. New evidence has emerged on when to initiate ART, optimal ART regimens, the management of HIV coinfection with tuberculosis and chronic viral hepatitis, and the management of ART failure. This evidence formed the basis for the new recommendations contained in the 2010 guidelines and summarized in the Rapid advice: Antiretroviral therapy for HIV infection in adults and adolescents (http://www.who.int/hiv/pub/arv/ rapid_advice_art.pdf). Consideration was given to the risks and benefits of implementing each recommendation, in addition to its acceptability, cost and feasibility. The guidelines incorporate the best available evidence within a framework that emphasizes the public health approach to the scaling up of quality HIV care and treatment.(1) The consensus recommendations encourage earlier diagnosis and earlier treatment, and promote the use of less toxic regimens and more strategic laboratory monitoring. It is critical that national ART programme and public health leaders consider these recommendations in the context of countries’ HIV epidemics, the strengths and weaknesses of health systems, and the availability of financial, human and other essential resources.(1) Care must be exercised to avoid undermining current treatment programmes, to protect access for the most at-risk populations, to achieve the greatest impact for the greatest number of people and to ensure sustainability. 4. Background
- 17. 9 Funding to support this work comes from the US President’s Emergency Plan for AIDS Relief (PEPFAR), The United Nations Joint Programme on HIV/AIDS Unified Budget and Workplan (UNAIDS UBW), and specific funds through staff time. Declaration of interest forms were collected from every member of each guidelines working group. Two declarations of interest were made. Dr Charles Holmes declared previous employment, which ceased in January 2008, by Gilead Sciences, largely for phase 1 studies of experimental ARVs. This interest was assessed by the WHO Secretariat as not sufficient to preclude Dr Holmes’ participation in this meeting. Dr Pedro Cahn acted as a member of the Peer Review Group and declared that he serves as advisory board member for Abbott, Bristol Myers Squibb, Tibotec, Merck, Avexa, Pfizer and Gilead. This interest was assessed by the WHO Secretariat as not sufficient to preclude Dr Cahn’s participation in this meeting. 5. Funding and declarations of interest
- 18. 10 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach The principles guiding the development of these recommendations were as follows: • to prioritize the best options for treatment of HIV infection and propose alternatives if the best option was not available; • to be clear when high-quality evidence supports a strong recommendation; • to be clear when low-quality evidence or an uncertain balance between risks and benefit supports a conditional recommendation; • to be both realistic and aspirational, recognizing the possibility for progressive implementation of the recommendations over the lifetime of these guidelines until 2012. 6. Guiding principles
- 19. 11 • To provide evidence-based recommendations outlining a public health approach to the delivery of ART for adults and adolescents, with a focus on settings with limited health systems capacity and resources. • To identify the most potent, effective and feasible first-line, second-line and subsequent treatment regimens as components of expanded national responses for HIV care. • To develop recommendations applicable to the majority of populations regarding the optimal timing of ART initiation, preferred first-line and second-line ARV regimens and improved criteria for ART switching, and to introduce the concept of third-line ART regimens. The target audiences are national treatment advisory boards, partners implementing HIV care and treatment, and organizations providing technical and financial support to HIV care and treatment programmes in resource-limited settings. 7. Objectives of the guidelines and target audience
- 20. 12 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach Throughout 2009, WHO worked to update the guidelines for Antiretroviral therapy for HIV infection in adults and adolescents: Recommendations for a public health approach through a series of coordinated efforts to review and synthesize new and emerging evidence on the optimal use of ART within a public health approach. This process was based on the preparation GRADE profiles, systematic and targeted reviews, risk-benefit analyses, technical reports and assessments of impact, feasibility and cost. All evidence documentation prepared for these guidelines is available on the 2009-2010 ART guidelines for adults and adolescents evidence map web page (http://www.who.int/hiv/topics/ treatment/evidence3/en/index.html). Preparatory work included the following: • GRADE profiles on when to start ART, what to use in first-line and second-line regimens and when to switch to second-line therapy. • Systematic and targeted reviews on: −− the management of HIV/hepatitis and HIV/TB coinfection; −− ART safety, toxicity and teratogenicity; −− the utility of CD4 count and viral load in monitoring ART; −− ART failure criteria; −− third-line ART; −− interactions between ARVs and opioids, and drugs used for the treatment of tuberculosis (TB), viral hepatitis and malaria. • Consultations with PLHIV. • A report on ART adherence. • A review of current ART guidelines from 26 countries. • Costing information based on studies of procurement and production of ARVs. • An impact assessment of the number of patients in need of treatment according to various CD4 count thresholds. • A feasibility analysis for the introduction of the proposed guidelines in Malawi. Search strategies employed in the systematic reviews, meta-analyses and GRADE profiles which were conducted by the Cochrane HIV/AIDS group followed methodology described in The Cochrane handbook for systematic reviews of interventions (Version 5.0.2; last updated September 2009, available at http://www.cochrane-handbook.org/. In reviews where data were not amenable to meta-analysis and/or GRADE profiles, systematic searches, using relevant key words and search strings, were conducted of electronic databases (Medline/Pubmed, Embase, CENTRAL), conference databases (Aegis, AIDSearch, NLM Gateway and hand searches) and clinical trial registers (http://clinicaltrials.gov/ www.controlled- trials.com www.pactr.org). This guideline revision is in accordance with procedures outlined by the WHO Guidelines Review Committee and is based on the GRADE approach to evidence review. The process involved four 8. Methodology and process
- 21. 13 separate working groups: the Internal WHO ART Guideline Working Group, the ART Guideline Drafting Group, the external ART Peer Review Panel and the full ART Guideline Review Committee. The composition of the groups was in accordance with WHO procedures for guideline development and included HIV experts, civil society representatives, programme managers, costing experts, guideline methodologists, epidemiologists, health economists, PEPFAR technical working group representatives, PLHIV community representatives, and WHO regional and country officers. Declarations of Interests were submitted by group participants. The work was coordinated by the Antiretroviral, Treatment and HIV Care team of the WHO Department of HIV/AIDS. The academic institutions that contributed to writing the guidelines were the Liverpool Medical School (UK), the South African Medical Research Council / South African Cochrane Centre (South Africa), the University of California, San Francisco / Cochrane Collaborative Review group on HIV/AIDS (USA), the University of New South Wales (Australia) and the University of Bern (Switzerland). Contributions were also received from the US Centers for Disease Control and Prevention (CDC), UNAIDS and the Global Fund to Fight AIDS, Tuberculosis and Malaria. Consultations were held with civil society networks including the Global Network of People Living with HIV (GNP+), the International Treatment Preparedness Coalition (ITCP) and the International Community of Women with HIV/AIDS (ICW). Group processes were managed as follows. The proposed recommendations were considered separately by the ART Guideline Working and Drafting Groups using a risk-benefit analysis tool consisting of a table exploring the following domains: existing and proposed recommendations, evidence for the outcomes deemed critical (mortality, disease progression and serious adverse events), risks and benefits of implementing the recommendations, acceptability, costs, feasibility, suggested ranking of recommendations (strong or conditional), gaps and research needs. The groups placed emphasis on concerns and important outcomes as voiced by PLHIV and on the critical need to maintain equity, access and coverage. The draft recommendations, GRADE profiles, risk-benefit analysis tables and supporting data were circulated to the ART Peer Review Panel for comment before convening the multidisciplinary ART Guideline Review Committee in October 2009. Following the release of Rapid advice in November 2009, successive drafts of the full guidelines were prepared and circulated to the ART Guideline Drafting Group and the external ART Peer Review Panel for comments. All responses were considered and addressed in the final draft. Disagreements were resolved in discussions. The guidelines will be disseminated as a paper-based handbook and electronically on the WHO web site. Regional and subregional meetings are planned to adapt these global recommendations to local needs and facilitate implementation. A plan will be developed to evaluate the implementation of the guidelines by users. A review of the guidelines is planned for 2012. There will be interim reviews as new evidence becomes available.
- 22. 14 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach Recommendations contained in the 2006 guidelines were based on levels of evidence from randomized clinical trials (RCTs), scientific studies, observational cohort data and, where insufficient evidence was available, expert opinion. Each recommendation was rated using the criteria described in Table 1, the letters A, B, and C representing the strengths of the recommendations and the numerals I, II, III and IV representing the quality of the evidence. Cost- effectiveness, acceptability and feasibility were not explicitly considered. Table 1. Assessment of evidence as used in the 2006 guidelines Strength of recommendation Level of evidence to make for recommendation A. Recommended − should be followed B. Consider − applicable in most situations C. Optional I. At least one randomized controlled trial with clinical, laboratory or programmatic end-points II. At least one high-quality study or several adequate studies with clinical, laboratory or programmatic end-points III. Observational cohort data, one or more case-controlled or analytical studies adequately conducted IV. Expert opinion based on evaluation of other evidence In the 2010 guidelines the development of a recommendation remains guided primarily by the quality of evidence using GRADE methodology. However, the GRADE approach includes the additional domains of the balance between risks and benefits, acceptability (values and preferences), cost and feasibility. Values and preferences may differ in regard to desired outcomes or there may be uncertainty about whether an intervention represents a wise use of resources. Furthermore, despite clear benefits, it may not be feasible to implement a proposed recommendation in some settings. Table 2. Assessment of strengths of recommendations as used in the 2010 guidelines Strength of recommendation Rationale Strong The panel is confident that the desirable effects of adherence to the recommendation outweigh the undesirable effects. 9. From evidence to recommendation
- 23. 15 Strength of recommendation Rationale Conditional The panel concludes that the desirable effects of adherence to a recommendation probably outweigh the undesirable effects. However: the recommendation is only applicable to a specific group, population or setting OR new evidence may result in changing the balance of risk to benefit OR the benefits may not warrant the cost or resource requirements in all settings. No recommendation possible Further research is required before any recommendation can be made. In the GRADE approach, the quality of a body of evidence is defined as the extent to which one can be confident that the reported estimates of effect (desirable or undesirable) available from the evidence are close to the actual effects of interest. The usefulness of an estimate of the effect of an intervention depends on the level of confidence in that estimate. The higher the quality of evidence, the more likely a strong recommendation can be made. It is not always possible to prepare GRADE profiles for all interventions. Table 3. Assessment of strength of evidence as used in the 2010 guidelines Evidence level Rationale High Further research is very unlikely to change confidence in the estimate of effect. Moderate Further research is likely to have an important impact on confidence in the effect. Low Further research is very likely to have an estimate of effect and is likely to change the estimate. Very low Any estimate of effect is very uncertain.
- 24. 16 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach Table 4. Additional domains considered in developing strengths of recommendations Domain Rationale Benefits and risks When developing a new recommendation, desirable effects (benefits) need to be weighed against undesirable effects (risks), considering any previous recommendation or an alternative. The larger the gap or gradient in favour of the benefits compared to the risks, the more likely a strong recommendation will be made. Values and preferences (acceptability) If the recommendation is likely to be widely accepted or valued more highly, a strong recommendation will probably be made. If there is a great deal of variability or if there are strong reasons that the recommended course of action is unlikely to be accepted, it is more probable that a conditional recommendation will be made. Costs / financial implications (resource use) Lower costs (monetary, infrastructure, equipment or human resources), or greater cost-effectiveness will more probably result in a strong recommendation. Feasibility If an intervention is achievable in a setting where the greatest impact is expected to be attained, a strong recommendation is more probable. Tools have been developed to assist national ART advisory committees when assessing the feasibility of implementing a new recommendation. These are available at: http://www.who. int/hiv/topics/treatment/evidence3/en/index.html
- 25. 17 WHO normative guidelines are developed for a global audience and it is expected that each country will adapt the recommendations to suit its own circumstances. WHO endorses the use of a national technical or advisory treatment working group to direct the adaptation process. It is recognized that the implementation of some recommendations may be challenging in some settings in view of the differing prevalence of HIV and of limited available and promised resources. It is recognized that the new recommendations have the potential to increase substantially the number of people eligible for ART and to increase the cost of delivering ART as part of comprehensive care. Immediate and full implementation of these recommendations may not be practicable, feasible or affordable. However, country-level strategic planning should be directed towards eventually implementing these recommendations and achieving national universal access to HIV care and treatment. It is recommended that national ART advisory committees consider the following six guiding principles to direct decision-making when introducing the revised recommendations. 1. Do no harm Seek to maintain current progress of treatment programmes without disrupting the care of those on treatment or compromising PLHIV at highest risk for poor outcomes. 2. Accessibility Ensure that all clinically eligible people infected with HIV are able to enter treatment services. 3. Quality of care Ensure that care achieves the highest standards possible. 4. Equity of access Ensure fairness and justice in access to treatment services. 5. Efficiency in resource use Aim to achieve the greatest health impact with the optimal use of available human and financial resources. 6. Sustainability Understand the long-term consequences of changes and have the vision to provide continued, lifelong access to ART for those in need. While the six guiding principles should be used to direct decision-making, contextual issues must also be taken into consideration, and it is not expected that all national ART advisory committees will come to the same decisions. It is important to engage stakeholders, including PLHIV, civil society and health-care workers, in open discussions about how to make choices and implement changes. In addition, the following points should be considered. 10. Adapting the guidelines
- 26. 18 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach 1. Strengthen health systems In making decisions, priority should be given to interventions that will directly or indirectly strengthen health systems. 2. Implement in phases It may not be possible to implement every new recommendation in every setting. A phased approach may be necessary if only some recommendations can be implemented. 3. Understand the perspectives of PLHIV The toxicity of d4T is of concern to the majority of PLHIV and its continuing use may undermine confidence in ART. If d4T has to be included in ongoing regimens, strategies should be devised to allow for substituting an alternative drug in cases of toxicity. There should be a plan to eventually avoid the routine use of this drug. 4. Be forward-looking The WHO guideline Antiretroviral therapy for HIV infection in adults and adolescents will next be updated in 2012. Member States should strive to adopt the 2010 recommendations before that date. An adaptation guide has been written to accompany these guidelines. WHO recognizes that the new recommendations will promote significant benefits to HIV-infected individuals, and also that they have the potential to substantially increase the number of people in need of ART and the cost of delivering it. Depending on how the new guidelines are implemented or interpreted, they could also lead to unintended consequences, such as reduced access to those most in need or the undermining of existing ART coverage or impending ongoing or planned research. The purpose of the adaptation guide is to assist Member States and programme managers to choose and prioritize the recommendations, especially where resources are limited. In addition, the guide is intended to serve as an advocacy tool for policy-makers and to provide a basis for difficult choices and decisions in Member States. The adaptation guide is available at: http://www.who.int/hiv/topics/treatment/guide_for_adaptation.pdf. To further assist countries, programme managers, academic institutions and national ART advisory committees to adapt these new recommendations to their local circumstances, the following materials are available on the WHO main evidence map web page. http://www.who.int/ hiv/topics/treatment/evidence3/en/index.html.
- 27. 19 Earlier initiation of ART On the basis of the available evidence the panel recommended ART initiation for all PLHIV with a CD4 count of ≤350 cells/mm3 and for those with WHO clinical stage 3 or 4 if CD4 testing is not available. Simplified, less toxic antiretroviral drugs for use in first-line and second-line therapy While current options have permitted rapid ART scale-up, the cost in terms of side-effects has been considerable. There is a clear demand both from PLHIV and health-care providers to phase in less toxic ARVs while maintaining simplified fixed-dose combinations. The available evidence indicates that initial ART should contain an NNRTI (either NVP or EFV) plus two NRTIs, one of which should be 3TC or FTC and the other AZT or TDF. Countries are advised to choose one second-line regimen for individuals with first-line failure. Promoting the initiation of ART for all those with HIV/TB coinfection While recognizing that this recommendation will be challenging for many countries with a significant HIV and TB burden, the panel placed high value on reducing the impact of TB on societies and on the data demonstrating a reduction in all-cause mortality among individuals provided with TB therapy and ART. Promoting improved HBV diagnosis and more effective treatment of HIV/HBV coinfection Evidence supports the initiation of ART, irrespective of WHO disease stage or CD4 cell count, for all those with HIV/HBV coinfection and chronic active hepatitis B when treatment is indicated for hepatitis B. However, there is no agreed definition of chronic active hepatitis in resource-limited settings. Despite this, the panel felt that it was necessary to include the principles of optimum care for those with HIV/HBV coinfection and bring these into alignment with recommendations in well-resourced settings. There is an urgent need to develop diagnostic criteria to identify individuals with HIV/HBV coinfection who need treatment in situations where HBV DNA and liver biopsy are not routinely available. More strategic monitoring for antiretroviral efficacy and toxicity While laboratory monitoring should not be a barrier to initiating ART, the newly recommended ARV regimens may require more laboratory monitoring than current regimens, especially in individuals at higher risk for adverse events. A phased-in approach to the use of viral load testing, if feasible, will improve the identification of treatment failure. 11. Summary of changes
- 28. 20 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach When to start All adolescents and adults including pregnant women with HIV infection and CD4 counts of ≤350 cells/mm3, should start ART, regardless of the presence or absence of clinical symptoms. Those with severe or advanced clinical disease (WHO clinical stage 3 or 4) should start ART irrespective of their CD4 cell count. What to use in first- line therapy First-line therapy should consist of an NNRTI + two NRTIs, one of which should be zidovudine (AZT) or tenofovir (TDF). Countries should take steps to progressively reduce the use of stavudine (d4T) in first-line regimens because of its well-recognized toxicities. What to use in second-line therapy Second-line ART should consist of a ritonavir-boosted protease inhibitor (PI) plus two NRTIs, one of which should be AZT or TDF, based on what was used in first-line therapy. Ritonavir-boosted atazanavir (ATV/r) or lopinavir/ritonavir (LPV/r) are the preferred PIs. Laboratory monitoring All patients should have access to CD4 cell–count testing to optimize pre-ART care and ART management. HIVRNA (viral-load) testing is recommended to confirm suspected treatment failure. Drug toxicity monitoring should be symptom-directed. HIV/TB coinfection Irrespective of CD4 cell counts, patients coinfected with HIV and TB should be started on ART as soon as possible after starting TB treatment. HIV/HBV coinfection Irrespective of CD4 cell counts or WHO clinical stage, patients who require treatment for HBV infection should start ART. First-line and second-line regimens for these individuals should contain TDF and either emtricitabine (FTC) or lamivudine (3TC). 12. Recommendations at a glance
- 29. 21 Table 5. When to start antiretroviral therapy Target population 2010 ART guideline 2006 ART guideline HIV+ asymptomatic ARV-naive individuals CD4 ≤350 cells/mm3 CD4 ≤200 cells/mm3 HIV+ symptomatic ARV-naive individuals WHO clinical stage 2 if CD4 ≤350 cells/mm3 OR WHO clinical stage 3 or 4 irrespective of CD4 cell count WHO stage 2 or 3 and CD4 ≤200 cells/mm3 WHO stage 3 if CD4 not available WHO stage 4 irrespective of CD4 cell count Consider treatment for WHO clinical stage 3 and CD4 cell count between 200 and 350 cells/mm3 HIV+ pregnant women CD4 ≤350 cells/mm3 irrespective of clinical symptoms OR WHO clinical stage 3 or 4 irrespective of CD4 cell count WHO stage 1 or 2 and CD4 ≤200 cells/mm3 WHO stage 3 and CD4 ≤350 cells/ mm3 WHO stage 4 irrespective of CD4 count HIV/TB coinfection ARV-naive individuals Presence of active TB disease, irrespective of CD4 cell count Presence of active TB disease and CD4 ≤350 cells/mm3 ART Initiation can be delayed if CD4 ≥200 cells/mm3 HIV/HBV coinfection ARV-naive individuals Individuals who require treatment for their HBV infection*, irrespective of CD4 cell count No specific recommendation * The current diagnosis of chronic active hepatitis in well-resourced settings is based on histological parameters obtained by liver biopsy and/or the availability of HBV DNA testing, neither of which is usually available in resource-limited settings. A global definition of chronic active hepatitis in the context of resource-limited settings based on clinical signs and simpler laboratory parameters is under discussion.
- 30. 22 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach Table 6. What antiretroviral therapy to start Target population 2010 ART guideline 2006 ART guideline HIV+ ARV-naive adults and adolescents No change, but in settings where d4T regimens are used as the principal option for starting ART a progressive plan to move towards AZT-based or TDF-based first-line regimens should be developed, based on an assessment of cost and feasibility AZT or TDF + 3TC (or FTC) + EFV or NVP HIV+ pregnant women AZT preferred but TDF acceptable EFV included as a NNRTI option (but do not initiate EFV during first trimester) Benefits of NVP outweigh risks where CD4 count is 250−350 cells/mm3 In HIV+ women with prior exposure to MTCT regimens, see ART recommendations in section 13.2 AZT + 3TC + NVP HIV/TB coinfection No change ART should be initiated as soon as possible in all HIV/TB-coinfected patients with active TB (within 8 weeks after the start of TB treatment) AZT or TDF + 3TC (or FTC) + EFV HIV/HBV coinfection NNRTI regimens that contain both TDF + 3TC (or FTC) are required TDF + 3TC (or FTC) + EFV Table7. Recommended second-line antiretroviral therapy Target population 2010 ART guideline* 2006 ART guideline HIV+ adults and adolescents If d4T or AZT used in first-line therapy TDF + 3TC (or FTC) + ATV/r or LPV/r ABC + ddI or TDF+ ABC or ddI +3TC or TDF + 3TC (± AZT) plus ATV/r or FPV/r or IDV/r or LPV/r or SQV/r If TDF used in first-line therapy AZT + 3TC (or FTC) + ATV/r or LPV/r
- 31. 23 Target population 2010 ART guideline* 2006 ART guideline HIV+ pregnant women Same regimens as recommended for adults and adolescents ABC + ddI or TDF+ ABC or ddI +3TC or TDF + 3TC (± AZT) plus LPV/r or NFV or SQV/r HIV/TB coinfection If rifabutin available (150 mg 3 times/ week) Same regimens as recommended for adults ABC + ddI or TDF+ ABC or ddI +3TC or TDF + 3TC (± AZT) plus LPV/r or SQV/r with adjusted dose of RTV (LPV/r 400 mg/400 mg twice a day or LPV/r 800 mg/200 mg twice a day or SQV/r 400 mg/400 mg twice a day) If rifabutin not available Same NRTI backbones recommended for adults plus LPV/r or SQV/r with adjusted dose of RTV (LPV/r 400 mg/400 mg twice a day or LPV/r 800 mg/200 mg twice a day or SQV/r 400 mg/400 mg twice a day) HIV/HBV coinfection AZT + TDF + 3TC (or FTC) + ATV/r or LPV/r 3TC- and/or TDF-containing regimens * ABC and ddI can be considered as backup options in case of AZT or TDF toxicity or if AZT or TDF are contraindicated.
- 32. 24 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach 13.1. Recommendations 1. It is recommended to treat all patients with CD4 counts of ≤350 cells/mm3 irrespective of the WHO clinical stage. (Strong recommendation, moderate quality of evidence) 2. It is recommended that all patients with WHO clinical stage 1 and 2 should have access to CD4 testing to decide when to initiate treatment. (Strong recommendation, low quality of evidence) 3. It is recommended to treat all patients with WHO clinical stage 3 and 4 irrespective of CD4 count. (Strong recommendation, low quality of evidence) In making these recommendations, the ART Guideline Review Committee (the “panel”) placed high value on avoiding death, disease progression and the likely risk of HIV transmission over and above cost and feasibility. 13.2. Evidence The evidence used in formulating recommendations on when to start ART comes from a systematic review: Optimal time of initiation of antiretroviral therapy for asymptomatic, HIV- infected, treatment-naive adults.(2) The review included randomized controlled clinical trials (RCTs) and cohort studies, in which ART initiation was stratified according to CD4 cell count. On the basis of GRADE methodology, the evidence was rated for each of the critical and important outcomes to determine whether or not to change the current WHO guideline. The recommendations are supported by moderate quality evidence for critical patient and public health outcomes from one unpublished RCT and one post hoc analysis nested in an RCT. In the GRADE evidence profile, pooled data from these two studies provide moderate evidence that starting ART at CD4 levels higher than 200 or 250 cells/mm3 reduces mortality rates in asymptomatic, ART-naive, HIV-infected people. The panel also reviewed large observational data sets from both resource-limited and well-resourced settings that were consistent with data from the RCT, but these did not add to the overall quality of evidence. The panel considered the recommendations to be feasible if introduced in a phased manner, with the speed and completeness determined by health-system capacity, HIV burden, ART coverage, equity of access and funding. Recent modelling and observational data suggest that more than 50% of HIV-infected patients with WHO clinical stage 2 may have a CD4 count of ≤350 cells/mm3. However, considering the uncertain prognostic value of some WHO clinical stage 2 conditions, the panel recommended that HIV-infected individuals with WHO clinical stage 1 and 2 should have access to CD4 testing to decide if treatment should be initiated. 13. When to start
- 33. 25 13.3. Summary of findings Moderate-quality evidence supports strong recommendations for the timing of ART initiation for the critical outcomes of absolute risk of death, disease progression (including tuberculosis), and the occurrence of serious adverse events. One RCT specifically aimed to determine the optimal time to initiate ART in asymptomatic, treatment-naive, HIV-infected adults. The CIPRA HT-001 (2009) study, a single-centre trial in Haiti, randomized 816 ART-naive participants with a CD4 count of 200−350 cells/mm3, to receive early treatment (start ART within 2 weeks of enrolment) versus standard-of-care treatment (start ART when the CD4 count is <200 cells/mm3 or following the development of an AIDS-defining illness).(3) The median CD4 count at study entry was 280 cells/mm3 in the early treatment group and 282 cells/mm3 in the standard-of-care group. The primary study end-point was survival and the secondary end-point was incident TB. The Data Safety and Monitoring Board (DSMB) recommended cessation of the study after a median follow up of 21 months (1−44 months). Deaths and incident TB occurred in 6 and 18 patients respectively in the early group compared to 23 and 36 patients in the delayed group (mortality HR 4.0, p = 0.0011; incident TB HR 2.0, p = 0.0125). Of the participants in the standard-of-care group, 40% reached a CD4 cell count of <200 cells/ mm3, developed an AIDS-defining illness or died. Early ART initiation was examined further in one subgroup post hoc analysis (249 participants) nested in a larger RCT. The SMART trial was a multicentre study conducted at 318 sites in 33 high-income and low/middle-income countries, which randomized 5472 participants with CD4 cell counts of >350 cells/mm3 to either a viral suppression strategy (goal of maximal and continuous viral suppression) versus a drug conservation strategy (ART deferred until CD4 was <250 cells/mm3).(4) In a subset analysis of 477 patients who were ART-naive at study entry (n = 249) or who had not received ART for >6 months before randomization (n = 228) and who were randomized to start ART immediately (with CD4 of >350 cells/mm3) or delayed until after CD4 dropped to <250 cells/mm3, there was a reduction of disease progression and serious non-AIDS events when ART was initiated before the CD4 cell count dropped to ≤350 cells/mm3 compared with delaying until the CD4 count was <250 cells/mm3. In the GRADE profile, pooled data from this RCT and the subgroup post hoc analysis provided moderate evidence that starting ART at CD4 levels higher than 200 or 250 cells/mm3 reduced mortality rates in asymptomatic, ART-naive HIV-infected people. Evidence regarding a reduction in morbidity was less strong because there were few events. The numbers of adverse events were also small. As the CIPRA-HT001 2009 trial was conducted in a resource-limited setting, the applicability of these results in determining a change in WHO guidelines is high. The GRADE profile notes that the quality of these data was limited by imprecision (there was only one RCT), indirectness (the SMART data come from a post hoc subset analysis) and reporting bias (there may be other trials which did not conduct or publish similar analyses of potential subsets within the original trials).
- 34. 26 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach The results from the CIPRA HT-001 and SMART trials are consistent with four observational cohort studies from resource-limited and well-resourced countries, which showed that early initiation of ART was associated with reduced morbidity and mortality.(5−8) GRADE tables were not produced for the four observational studies identified in the systematic review as they would not have increased the overall quality of evidence. No trials were identified which evaluated the optimal timing of initiation of ART in people coinfected with hepatitis B, hepatitis C or both. 13.4. Benefits and risks Benefits Modelling estimates predict that the initiation of ART for individuals with a CD4 cell count of ≤350 cells/mm3 or with WHO clinical stage 3 or 4 will result in the numbers of people on ART increasing by 49% and a reduction in HIV-related mortality of 20% by 2010−2015.(9) Further modelling data suggest additional transmission benefit from earlier initiation of ART for both sexual transmission and MTCT of HIV providing that there is high treatment coverage and high adherence.(10) Earlier initiation and more time spent on ART may provide impetus to shift to less toxic first-line regimens and reduced prices for newer fixed-dose combinations (FDCs). Observational and RCT data confirm that there is an increased risk of TB and invasive bacterial diseases as CD4 cell counts decline.(11,12) Conversely, there is a 54% to 92% reduction in TB in individuals receiving ART.(13) Risks It is estimated that increasing the threshold for ART initiation can increase ART cost up to 57% by 2010−2015.(9) Broadening the criteria for treatment may result in some persons in urgent need of treatment being displaced by persons for whom treatment would be beneficial but not as urgent. In recommending a higher CD4 count threshold for initiation, a guiding principle is that those most in need of treatment should retain priority access. Earlier initiation will mean longer exposure to ART (estimated to be 1 to 2 years more) and the possibility of more ART-related side-effects and ARV resistance. It remains unclear if asymptomatic individuals will accept HIV testing or ART. Additionally, the impact of earlier initiation on adherence is uncertain. 13.5. Acceptability and feasibility In consultations with PLHIV, the benefits of starting ART earlier were recognized and strongly supported. However, concern was voiced about the increased risk of adverse events, resistance to first-line ARVs, drug stock-outs, and unavailability of second-line regimens. While earlier ART initiation will reduce the current disparity between treatment recommendations in resource-limited and well-resourced settings, it will appear to decrease treatment coverage. Ministries and donors may feel under pressure to address immediate increased costs. Feasibility will be enhanced if there is a phased introduction of the higher thresholds, with the speed and completeness determined by the health system’s capacity, HIV burden, ART coverage and funding.
- 35. 27 13.6. Clinical considerations Table 8. WHO clinical staging of HIV disease in adults and adolescents Clinical stage 1 Asymptomatic Persistent generalized lymphadenopathy Clinical stage 2 Moderate unexplained weight loss (under 10% of presumed or measured body weight) Recurrent respiratory tract infections (sinusitis, tonsillitis, otitis media, pharyngitis) Herpes zoster Angular cheilitis Recurrent oral ulcerations Papular pruritic eruptions Seborrhoeic dermatitis Fungal nail infections Clinical stage 3 Unexplained severe weight loss (over 10% of presumed or measured body weight) Unexplained chronic diarrhoea for longer than 1 month Unexplained persistent fever (intermittent or constant for longer than 1 month) Persistent oral candidiasis Oral hairy leukoplakia Pulmonary tuberculosis Severe bacterial infections (e.g. pneumonia, empyema, meningitis, pyomyositis, bone or joint infection, bacteraemia, severe pelvic inflammatory disease) Acute necrotizing ulcerative stomatitis, gingivitis or periodontitis Unexplained anaemia (below 8 g/dl ), neutropenia (below 0.5 x 109/l) and/or chronic thrombocytopenia (below 50 x 109/l)
- 36. 28 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach Clinical stage 4 HIV wasting syndrome Pneumocystis jiroveci pneumonia Recurrent severe bacterial pneumonia Chronic herpes simplex infection (orolabial, genital or anorectal of more than 1 month’s duration or visceral at any site) Oesophageal candidiasis (or candidiasis of trachea, bronchi or lungs) Extrapulmonary tuberculosis Kaposi sarcoma Cytomegalovirus disease (retinitis or infection of other organs, excluding liver, spleen and lymph nodes) Central nervous system toxoplasmosis HIV encephalopathy Extrapulmonary cryptococcosis including meningitis Disseminated nontuberculous mycobacteria infection Progressive multifocal leukoencephalopathy Chronic cryptosporidiosis Chronic isosporiasis Disseminated mycosis (histoplasmosis, coccidiomycosis) Recurrent septicaemia (including nontyphoidal Salmonella) Lymphoma (cerebral or B cell non-Hodgkin) Invasive cervical carcinoma Atypical disseminated leishmaniasis Symptomatic HIV-associated nephropathy or HIV-associated cardiomyopathy Source: Revised WHO clinical staging and immunological classification of HIV and case definition of HIV for surveillance. 2006.
- 37. 29 Table 9. Criteria for ART Initiation in specific populations Target population Clinical condition Recommendation Asymptomatic individuals (including pregnant women) WHO clinical stage 1 Start ART if CD4 ≤350 Symptomatic individuals (including pregnant women) WHO clinical stage 2 Start ART if CD4 ≤350 WHO clinical stage 3 or 4 Start ART irrespective of CD4 cell count TB and hepatitis B coinfections Active TB disease Start ART irrespective of CD4 cell count HBV infection requiring treatment* Start ART irrespective of CD4 cell count * The current standard definition of chronic active hepatitis in industrialized countries is mainly based on histological parameters obtained by liver biopsy, a procedure not usually available in the large majority of resource-limited settings. A global definition of chronic active hepatitis for resource-limited settings based on clinical and more simple laboratory parameters is under discussion. While increased access to CD4 testing is a priority, the lack of a CD4 cell count should not be a barrier to the initiation of ART. For ART programmes in many countries with the highest HIV burden, clinical criteria remain the basis for deciding when to initiate ART. In both resource- limited and well-resourced settings, there is a move towards earlier initiation of ART. However, many people still present for the first time with advanced HIV disease, with a CD4 count of <200 cells/mm3 or with an opportunistic infection.(14,15) Clinical assessment Clinical staging is intended for use where HIV infection has been confirmed by HIV antibody testing. It is used to guide decisions on when to start cotrimoxazole prophylaxis and when to start ART. Table 8 (WHO clinical staging of HIV disease in adults and adolescents) and Annex 21.5 (Diagnostic criteria for HIV-related clinical events in adults and adolescents) provide details of specific staging conditions and the criteria for recognizing them. For individuals with advanced HIV disease (WHO clinical stage 3 or 4), ART should be initiated irrespective of the CD4 cell count. Both stages 3 and 4 are independently predictive of HIV- related mortality.(16−19) Assessing the need for ART in those with WHO clinical stage 2 presents challenges. Some stage 2 conditions may be considered more indicative of HIV disease progression than others. For example, papular pruritic eruptions (PPEs) typically occur with CD4 counts of <200 cells/mm3, and most physicians would recommend the initiation of ART in the presence of PPEs and the absence of a CD4 count.(20,21) Conversely, recurrent oral ulceration or a fungal nail infection generally would not be considered triggers to start ART. Given the uncertainty with which stage 2 conditions predict mortality and disease progression, HIV-
- 38. 30 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach infected individuals with WHO clinical stage 2 should have priority access to CD4 testing to decide if treatment should be initiated. The same recommendation to promote CD4 testing applies to asymptomatic individuals (WHO stage 1). The objective is to identify those with a low CD4 count, are still well, but need to start ART. Immunological assessment Expanded provider-initiated testing and counselling (PITC) and voluntary counselling and testing (VCT), together with immunological assessment (CD4 testing), are critical to achieving the goals of earlier diagnosis and starting ART before people become unwell or present with their first opportunistic infection.(22) A CD4 cell count performed at entry into care or prior to ART initiation will guide the decision on when to start ART and serves as the baseline if CD4 testing is used for ART monitoring. ART should be commenced in individuals with a CD4 count of ≤350 cells/mm3. Absolute CD4 cell counts fluctuate within individuals and with intercurrent illnesses. If feasible, CD4 testing should be repeated if a major management decision rests on the value, rather than using a single value. Serial CD4 measurements are more informative than individual values because they reflect trends over time. The total lymphocyte count (TLC) is no longer recommended to guide treatment decisions in adults and adolescents. Virological assessment In resource-limited settings, plasma viral load (HIVRNA) measurement is not required before the initiation of ART. However, expanded access to viral load testing is needed to improve the accuracy of diagnosing treatment failure. Earlier detection of virological failure allows both targeted adherence interventions and better preservation of the efficacy of second-line regimens.(23)
- 39. 31 14.1. Recommendations Start one of the following regimens in ART-naive individuals eligible for treatment. • AZT + 3TC + EFV • AZT + 3TC + NVP • TDF + 3TC (or FTC) + EFV • TDF + 3TC (or FTC) + NVP (Strong recommendation, moderate quality of evidence) Because stavudine (d4T) is relatively inexpensive and is currently a component of first-line therapy in many countries, the panel specifically considered studies of d4T-based regimens. In making these recommendations, the panel placed high value on avoiding the disfiguring, unpleasant and potentially life-threatening toxicity of d4T, in addition to the selection of regimens suitable for use in most patient groups, treatment durability and the benefits of using fixed-dose combinations. The available information suggests that abacavir (ABC) and didanosine (ddI) have serious constraints for use in first-line regimens (toxicities and cost) and the panel focused on comparisons between AZT, TDF and d4T-based regimens. 14.2. Evidence Using Cochrane systematic review methodology, triple-drug ARVs for the initial treatment of HIV infection were examined in RCTS, other controlled trials, and cohort and case-control studies. The comparisons of interest were mortality, disease progression, virological response to ART (the proportion of individuals who suppressed viral replication to undetectable levels, defined as <40, <400 or <500 copies/ml), serious adverse events (Division of AIDS adverse event toxicity scale, National Institute of Allergy and Infectious Diseases, USA, 2004), adherence, tolerability and retention, and immunological response to ART (median or mean change in CD4 cell count from baseline). The quality of evidence was assessed using GRADE evidence profiles. The following specific interventions were compared: • dual NRTI backbone with d4T versus dual NRTI backbone with AZT; • dual NRTI backbone with TDF versus dual NRTI backbone with AZT or d4T; • 2 NRTIs + NVP versus 2 NRTIs + EFV. Current evidence suggests that the new recommended regimens are comparable in terms of efficacy, with a better overall toxicity profile than d4T-based regimens. The panel was reassured by the GRADE evidence profile from RCTs, non-randomized trials and observational studies from low-income and middle-income countries, which indicate no superiority for the outcomes of interest of AZT over TDF, or of NVP over EFV as part of combination ART for treatment-naive individuals. 14. What to start
- 40. 32 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach 14.3. Summary of main findings This systematic review did not find any evidence from RCTs, non-randomized trials or observational studies from resource-limited settings that clearly indicated the superiority of regimens based on AZT, d4T or TDF or the superiority of either EFV or NVP, in triple-drug antiretroviral regimens for treatment-naive patients. Studies which compared or are comparing AZT and d4T in different combinations provide reasonably robust evidence that AZT-containing and d4T-containing regimens are equivalent. (24−33) These studies have a variety of limitations and the overall GRADE evidence profile rating was very low. Five of the six studies were open-label, several studies compared AZT + 3TC to d4T + ddI, potentially obscuring the head-to-head comparison of AZT and d4T, and others used protease inhibitors as a third drug. The Adult Antiretroviral Treatment and Resistance Study (TSHEPO study) in Botswana is directly comparing combinations of AZT + 3TC + NVP or EFV and d4T + 3TC + NVP or EFV.(34) Three RCTs have compared regimens containing TDF to d4T or AZT. Two of these studies used 3TC as the second NRTI and allowed for direct comparisons (35,36); the third compared AZT + 3TC with TDF + FTC.(37) Two of these studies had equivalent findings; that efficacy and safety were similar for AZT + 3TC + EFV and d4T + 3TC + EFV, and for TDF + FTC + EFV and TDF + 3TC + EFV. (35,36) The third study compared TDF + 3TC to AZT +3TC, both with once-daily NVP, and was prematurely discontinued after failure of the TDF + 3TC + NVP arm to suppress viral replication in 8 of 35 participants(35,36). In two other small studies, similar rates of failure to suppress viral replication have also been found in patients receiving NVP once daily.(38,39) However, in the large ARTEN study, (atazanavir/ritonavir on a background of tenofovir and emtricitabine vs. nevirapine) in which 569 patients were randomized to receive NVP 200 mg BID, NVP 400 mg OD or ATV /r 300/100mg OD each given with TDF/FTC OD, non-inferiority of the primary end-point (undetectable VL at week 48) was established between the combined NVP arms and ATV/r arm. (40) Data from AIDS therapy evaluation in the Netherlands (ATHENA) and Swiss HIV cohort study (4471 on NVP twice-daily and 629 on NVP once-daily regimens) suggest that NVP once daily is at least as efficient as NVP prescribed twice daily.(41) Additional evidence comes from observational studies which were not included in the GRADE profile. None were conducted in low-income and middle-income settings. These studies showed that TDF-containing backbones were associated with a higher proportion of non-detectable viraemia,(42) a lower rate change due to toxicity,(43) overall greater durability (44) and slower rates of CD4-cell increase.(45,46) Two observational studies reported that TDF/FTC or 3TC was cost-saving compared to AZT+3TC.(47,48) Six RCTs which have compared NVP to EFV found no differences in efficacy.(49−54) One RCT reported that EFV was less likely than NVP to be associated with the development of antiretroviral resistance.(53) The GRADE evidence profile is moderate to high, with the exception of drug
- 41. 33 resistance, which was examined in only a single study. Ongoing studies will add substantially to this literature.(55−57) The systematic review of d4T safety and toxicity prepared for this guideline revision reported data from three RCTs and 24 observational studies, demonstrating the consistent association between d4T and peripheral neuropathy, lipoatrophy and lactic acidosis. 14.4. Benefits and risks Benefits Phasing in AZT and TDF will reduce the risk of acute d4T-related lactic acidosis and of long-term mitochondrial toxicities (particularly lipoatrophy and peripheral neuropathy), and has the potential for improved adherence and reduced lost to follow-up. TDF can be included in a once- daily FDC. The combination of TDF + 3TC or FTC is the recommended NRTI backbone in the presence of HBV coinfection. AZT + 3TC is a preferred NRTI backbone option in pregnant woman. There will be fewer within-class changes with more durable and safer regimens. Risks AZT and TDF may require more laboratory monitoring than d4T-based regimens. There may be concern from PLHIV and care providers about anaemia (AZT) and renal toxicity (TDF). There is uncertainty whether TDF requires renal screening and monitoring in all individuals or only in selected populations (elderly, those with low body weight, those taking concomitant renal toxic drugs or with diseases such as diabetes and hypertension). TDF has been reported as associated with bone mineral loss.(58) Recently, safety and effectiveness in adolescents was reviewed; individuals aged ≥12 years and weighing ≥35 kg should use the dose recommended in adults.(58) In addition to anaemia, AZT is associated with initial gastrointestinal adverse events, proximal myopathy and skin hyperpigmentation. Not all of these options are currently available as a full FDC (AZT + 3TC + EFV; TDF + 3TC + NVP; TDF + FTC + NVP). While progressive reduction in the use of d4T is occurring, it may be retained as an interim measure if plans are initiated to monitor and manage toxicity. In certain situations, d4T may be retained as a backup drug, such as when TDF and AZT are contraindicated. 14.5. Acceptability and feasibility As current evidence suggests that the recommended regimens are comparable in terms of efficacy, countries should select one of them as the preferred option for most patients initiating ART, on the basis of factors related to acceptability and feasibility, such as: • numbers of individuals needing to start ART according to 2010 and 2015 targets; • numbers of individuals starting ART who have HIV/TB coinfection or chronic active HIV/HBV coinfection; • anaemia (due to malaria, malnutrition, intestinal parasites, repeated pregnancies or other causes); • pregnant women or women of reproductive age;
- 42. 34 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach • predicted expenditure per person needing ART (based on selected national start criteria); • availability of FDC; • in-country cost of the drug regimens; • decisions by countries on laboratory requirements to monitor toxicities; • training needs for the introduction and management of the regimens; • countries may need to use modelling to assist in decision-making. Table 10. Preferred first-line ART in treatment-naive adults and adolescents Target population Preferred options Comments Adults and adolescents AZT or TDF + 3TC or FTC + EFV or NVP Select the preferred regimens applicable to the majority of PLHIV Use fixed-dose combinations Pregnant women AZT + 3TC + EFV or NVP Do not initiate EFV during first trimester TDF acceptable option In HIV women with prior exposure to PMTCT regimens, see ART recommendations in Table 11 HIV/TB coinfection AZT or TDF + 3TC or FTC + EFV Initiate ART as soon as possible (within the first 8 weeks) after starting TB treatment NVP or triple NRTIs are acceptable options if EFV cannot be used HIV/HBV coinfection TDF + 3TC or FTC + EFV or NVP Consider HBsAg screening before starting ART, especially when TDF is not the preferred first-line NRTI Use of two ARVs with anti-HBV activity required 14.6. The choice between NVP and EFV NVP and EFV have comparable clinical efficacy when administered in combination regimens. However, differences in toxicity profiles, the potential for interaction with other treatments, and cost should be considered when an NNRTI is being chosen.(54,59) NVP is associated with a higher incidence of rash, Stevens-Johnson syndrome, and hepatotoxicity compared to EFV.(54) The simultaneous initiation of NVP and other new drugs that can also cause rash (e.g. cotrimoxazole) should be avoided where possible. In the case of severe hepatic or skin reactions, NVP should be permanently discontinued and not restarted. NVP is the
- 43. 35 preferred NNRTI for women if there is potential for pregnancy or during the first trimester of pregnancy. While there are conflicting data regarding an increased risk of hepatic toxicity in women with CD4 counts between 250 and 350 cells/mm3, the panel found that there was limited evidence to cause concern but still urged caution in the use of NVP in women with CD4 counts of >250 cells/mm3 or in those with unknown CD4 cell counts. Close clinical monitoring (and laboratory monitoring if feasible) during the first 12 weeks of therapy is recommended when NVP is initiated in women with a CD4 cell count of 250−350 cells/mm3. EFV can be used once daily, is generally well tolerated but is more costly and currently less widely available than NVP. Its primary toxicities are related to the central nervous system (CNS) and possible, but not proven teratogenicity, if received during the first trimester of pregnancy (but not in the second and third trimesters), and rash. Rash is generally mild and self-resolving and usually does not require the discontinuation of therapy. The CNS symptoms are common. While they typically resolve after 2−4 weeks, they can persist for months, resulting in discontinuation of the drug. EFV should be avoided in patients with a history of severe psychiatric illness, when there is a potential for pregnancy (unless effective contraception can be assured) and during the first trimester of pregnancy. EFV is the NNRTI of choice in individuals with TB/HIV coinfection who are receiving rifampicin-based TB therapy. There are clinical situations when individuals need to replace EFV with NVP. The most common scenarios are when patients temporarily change from NVP to EFV because they need to take rifampicin-containing TB treatment and subsequently switch back to NVP on completion of TB treatment, and individuals with persistent EFV CNS intolerance. In this case, EFV can be stopped and full-dose NVP (200 mg twice daily) can be started immediately. There is no need for lead-in NVP dosing.(60,61) 14.7. AZT + 3TC + EFV option In recommending this as a preferred first-line regimen, the panel placed high value on the utility of EFV in the treatment of HIV/TB coinfection. Efficacy and safety Low (for AZT) to moderate (for EFV) GRADE evidence profiles for the critical outcomes of mortality, clinical progression and serious adverse events support this option. In the systematic review of AZT toxicity, low body mass and low CD4 cell count were independent predicators of developing AZT-induced anaemia.(62,63) Background rates of anaemia vary considerably. Malaria, pregnancy, malnutrition and advanced HIV disease are well-recognized risk factors for anaemia. The prevalence, incidence and predictors of severe anaemia with AZT- containing regimens in African adults were assessed in the Development of antiretroviral therapy in Africa (DART) trial.(63) More than 6% of individuals receiving AZT developed grade 4 (ACTG toxicity grading scale) anaemia by 12 months. In data from nine PEPFAR focus countries, 12% stopped AZT because of anaemia or gastrointestinal intolerance.(64) In Uganda, 25% of 1029 patients who initiated a d4T-containing ART were switched to AZT because of d4T toxicity,(65) and 5% subsequently switched to another drug because of AZT toxicity.
- 44. 36 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach The EFV toxicity review showed consistent reports of self-limiting or tolerable CNS adverse events and uncertainties about teratogenic risk in humans. In the important outcome (as distinct from the predetermined critical outcomes of mortality, disease progression and adverse events) of ARV resistance, EFV may be superior to NVP.(66) EFV should not be initiated in the first trimester of pregnancy but may be initiated in the second and third trimesters. There is conflicting evidence of very low quality on the risks of EFV causing neural tube defects. The overall rates of birth defects reported in association with EFV, NVP, LPV/r or TDF appear similar and are consistent with rates reported in congenital defects registries from general populations. However, neural tube birth defects are rare, with an incidence 0.1% in the general population. Prospective data are currently insufficient to provide an assessment of neural tube defect risk with first-trimester exposure, except to rule out a potential tenfold or higher increase in risk (i.e. an increase in risk from 0.1% to >1%). Since neural tube closure occurs by approximately 28 days of gestation and very few pregnancies are recognized by this time, the potential risk with the use of EFV in women who might conceive while receiving the drug is difficult to estimate. Women who are planning to become pregnant or who may become pregnant should use a regimen that does not include EFV, in order to avoid the highest risk period of exposure in utero (conception to day 28 of gestation). If a woman is diagnosed as pregnant before 28 days of gestation, EFV should be stopped and substituted with NVP or a PI. If a woman is diagnosed as pregnant after 28 days of gestation, EFV should be continued. There is no indication for termination of pregnancy in women exposed to EFV in the first trimester of pregnancy. Risk, benefits and acceptability AZT requires twice daily dosing and currently there is no AZT-containing triple-drug FDC (a dual FDC containing AZT + 3TC is available). Potentially troublesome AZT toxicities, such as proximal myopathy, gastrointestinal intolerance, skin hyperpigmentation and lipodystrophy, are not uncommon. EFV is preferred in individuals taking rifampicin-containing TB treatment. EFV is not approved in children under 3 years of age (and there are insufficient data on appropriate dosing for that age group). Recent single-dose NVP for the prevention of mother-to-child transmission (PMTCT) may compromise response to EFV because of cross-resistance. EFV is associated with CNS adverse events, which are common. 14.8. AZT + 3TC + NVP option In recommending this as a preferred first-line regimen, the panel placed high value on it as the preferred option in pregnancy. It is widely available, there is extensive experience in its use and the cost is lower than an EFV-containing regimen. Efficacy and safety NVP may be inferior to EFV in the important, noncritical outcome of ARV resistance (as distinct from the predetermined critical outcomes of mortality, disease progression and serious adverse events).(53) Based on safety concerns raised in some of these studies, the US FDA has cautioned
- 45. 37 against the use of NVP in women with high CD4 cell counts. This current review of NVP safety in women with CD4 counts of 250−350 cells/mm3 did not confirm an increased risk of serious adverse events. Available evidence is based largely on retrospective reviews or open-label studies, with one RCT and two post hoc analyses within an RCT (2NN study) informing the evidence profile. (54,67) The data are conflicting, with increased rates of hepatotoxicity and hypersensitivity reported in some studies (54,67−72) and not in others.(73−80) Two of these trials were in pregnant women. Other studies reported no difference in adverse events between those with low and high CD4 cell counts in virologically suppressed patients switching to NVP.(76,81,82) These studies support the concept that a suppressed viral load is a protective factor for NVP-related hypersensitivity in the situation where patients need to switch from an EFV-based (or PI-based) regimen to NVP. While there is a good representation of studies in resource-limited settings, the key recommendation regarding cautious use of NVP in the presence of higher CD4 cell counts is from high-income and middle-income settings.(54) An increased risk of hypersensitivity and hepatoxicity has been reported in men with a CD4 count of >400 cells/mm3.(83) The panel found that there was limited evidence to cause concern about the use of NVP in women with CD4 counts of 250−350 cells/mm3 but urged caution in the use of NVP in women with CD4 counts of >250 cells/mm3 or in those with unknown CD4 cell counts. The panel concluded that the benefits of using NVP in this situation outweigh the risks of not initiating ART but still urged close clinical monitoring (and laboratory monitoring if feasible) during the first 12 weeks of therapy when NVP is initiated in women with a CD4 cell count of 250−350 cells/mm3 or with an unknown CD4 cell count and in men with a CD4 cell count of >400 cells/mm3 or with an unknown CD4 cell count. Risk, benefits and acceptability The regimen is widely available, applicable to paediatric and adult populations and a preferred option in pregnancy, and there is large programmatic experience. Triple FDC formulations are available for adults and children. Some countries have moved to or are considering this combination already. PLHIV want low pill-burden and FDC options, but AZT and NVP adverse events may be unacceptable. NVP-associated hepatotoxicity /skin rash can be life-threatening (but there is an unclear relationship with CD4 and gender). Rifampicin and NVP drug-drug interactions are such that the combination should not be used unless no alternative is available. The NVP lead-in dose adds complexity. Recent single-dose NVP (sdNVP) use for PMTCT may compromise virological response.(84) 14.9. TDF + 3TC (or FTC) + EFV option In recommending this as a preferred regimen, the panel placed high value on the simplicity of use (potential for one pill once daily) and the treatment of HIV/HBV coinfection. Efficacy and safety The GRADE evidence profiles summarize evidence of low (for TDF) and moderate (for EFV) quality supporting the use of TDF + 3TC (or FTC) + EFV for the critical outcomes of mortality, clinical progression and serious adverse events. Existing TDF toxicity data suggest low rates of
- 46. 38 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach renal toxicity in prescreened patients. However, baseline rates of renal disease in African patients seem to be higher than in non-African populations. The GRADE evidence profile produced for this guideline revision demonstrated no difference in the occurrence of adverse events (changes in creatinine, proteinuria, all grade 3 or 4 adverse events or treatment discontinuation) in patients using TDF-containing regimens compared to other regimens. Imprecision (one pharmacokinetic study) and study limitations (small sample size) were reported in the profile. The cumulative incidence of nephrotoxicity in TDF-containing regimens has been reported as 1% to 4%, and the rate of Fanconi’s syndrome as 0.5% to 2.0%, with no association between renal disease and gender, age or race.(85,86) Only one study (open-label, 86 participants) reported data from resource-limited settings (Argentina, Brazil, Dominican Republic), with no discontinuations attributable to renal adverse events.(87) A 2007 report of all postmarketing adverse drug reactions up to April 2005 for 10 343 patients in developed countries using TDF reported observations of renal serious adverse events in 0.5% of individuals and graded elevations of serum creatinine in 2.2%. Risk factors for increased serum creatinine were concomitant nephrotoxic medications, elevated serum creatinine, low body weight, advanced age and lower CD4 cell count. One study of 15 pregnant women with limited treatment options reported creatinine clearance of >90 ml/min in all but one, who had a transient decline.(88) Risk, benefits and acceptability A triple FDC is available with low pill-burden (one pill once daily) which is well accepted by PLHIV. Two drugs in the regimen are active against HBV, no lead-in dosing is required, and the combination can be used in patients receiving rifampicin-containing TB treatment. There are limited data on the use of TDF without renal screening or monitoring in resource-limited settings. TDF is not approved in children and adolescents and there are limited data on the safety of TDF in pregnancy. Clinicians may have concerns about TDF use without renal monitoring, especially in individuals at higher risk for renal complications. There will be additional cost if laboratory monitoring of creatinine is required. The regimen may only be feasible where renal screening is available or not a prerequisite. An alternative non-EFV-containing regimen is required in the context of the first trimester of pregnancy or for women seeking to become pregnant. 14.10. TDF + 3TC (or FTC) + NVP option In recommending this as a preferred first-line regimen, the panel placed high value on lower cost compared to EFV-containing regimens and the treatment of HIV/HBV coinfection. Efficacy and safety TDF and NVP are discussed in previous sections.
- 47. 39 Risk, benefits and acceptability Two drugs in the regimen are active against HBV. There is a relatively low pill burden and the potential for a once-daily regimen. There is limited programmatic experience with this combination and there have been reports of higher rates of virological failure when compared to TDF + 3TC or FTC + EFV.(53) 14.11. Triple NRTI option It is recommended that the triple nucleoside regimens AZT + 3TC + ABC or AZT + 3TC + TDF should be used for individuals who are unable to tolerate or have contraindications to NNRTI- based regimens, particularly in the following situations: • HIV/TB coinfection; • pregnant women; • chronic viral hepatitis B; • HIV-2 infection. (Conditional recommendation, low quality of evidence) These two triple NRTI regimens may be considered as alternative first-line treatments in situations such as intolerance to both NNRTIs, or where an NVP-containing regimen is contraindicated and EFV is not available, in coinfection with TB or chronic hepatitis B, or in HIV-2 infection. Recent data from the DART trial, where the large majority of patients are taking AZT + 3TC + TDF, showed good clinical response and survival rates of around 90% over 5 years of follow-up.(63) However, some specific triple NRTI combinations, such as ABC + 3TC + TDF and TDF + ddI + 3TC, showed high rates of virological failure and should not be used. In HIV-2 infection, some studies suggest a higher risk of virological failure with the triple nucleoside regimen of AZT + 3TC + ABC when compared with boosted PI regimens. 14.12. Stavudine (d4T) In resource-limited settings, d4T continues to play a critical role in the scaling up of ART, where approximately 56% of HIV regimens still contain d4T.(89) Alternative options (AZT and TDF) are more expensive, require more laboratory monitoring and have higher initial discontinuation rates.(35,90) Cumulative exposure to d4T has the potential to cause disfiguring, painful and life- threatening side-effects, such as lipodystrophy, peripheral neuropathy and lactic acidosis. (91,92) Studies have identified several risk factors associated with d4T-related adverse events. Peripheral neuropathy was significantly associated with older age (over 35 or 40 years).(93−95) Lipodystrophy and hyperlactataemia were significantly associated with BMI >25 and female gender.(93,96,97) Female gender and high baseline weight were also significantly related to symptomatic hyperlactataemia/lactic acidosis and lipodystrophy in South Africa.(98)
- 48. 40 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach On the issue of progressive reduction in the use of d4T in settings where d4T regimens are used as the principal option for starting ART, countries should develop a plan to move towards AZT- based or TDF-based first-line regimens, on the basis of an assessment of cost and feasibility. Systems to prevent, monitor and manage d4T-related toxicities should be implemented. Safer but currently more expensive first-line ARTs should be progressively introduced as currently they may not be feasible or affordable in many high-burden settings with low coverage, less developed health systems, limited laboratory capacity, finite budgets and competing health priorities. In countries with high coverage and more developed health systems, transition to new treatment regimens should occur sooner. If d4T use is continued, it should be dosed at 30 mg BID for all individuals, irrespective of body weight.(99) 14.13. NRTIs not to be used together Certain dual NRTI backbone combinations should not be used in three-drug therapy. These are d4T + AZT (proven antagonism), d4T + ddI (overlapping toxicities) and 3TC + FTC (interchangeable, but should not be used together). The combinations of TDF + 3TC + ABC and TDF + 3TC + ddI select for the K65R mutation and are associated with high incidences of early virological failure. The combinations of TDF + ddI + any NNRTI are also associated with high rates of early virological failure and should be avoided.
- 49. 41 15.1. Recommendations for HIV-infected pregnant women 1. Start ART in all pregnant women with HIV and a CD4 count of ≤350 cells/mm3, irrespective of clinical symptoms. (Strong recommendation, moderate quality of evidence) 2. CD4 testing is required to determine if pregnant women with HIV and WHO clinical stage 1 or 2 disease need to start ARV treatment or ARV prophylaxis for PMTCT. (Strong recommendation, low quality of evidence) 3. Start ART in all pregnant women with HIV and WHO clinical stage 3 or 4, irrespective of CD4 count. (Strong recommendation, low quality of evidence) 4. Start one the following regimens in ART-naive pregnant women eligible for treatment: • AZT + 3TC + EFV; • AZT + 3TC + NVP; • TDF + 3TC (or FTC) + EFV; • TDF + 3TC (or FTC) + NVP. (Strong recommendation, moderate quality of evidence) 5. Do not initiate EFV during the first trimester of pregnancy. (Strong recommendation, low quality of evidence) In making these recommendations, the ART and PMTCT panels placed high value on ensuring that treatment begins early for pregnant women with HIV, improving maternal and child-health outcomes and avoiding MTCT, over and above concerns about cost or feasibility. When to start On the question of when to start, no studies specific to pregnant women were identified in the systematic review prepared for this guideline revision. Evidence from the general population supports strong recommendations for the timing of initiation in terms of reduction of mortality, disease progression, serious adverse events, the risk of TB and the risk of HIV transmission (sexual and mother to child). As with the recommendation on when to start in the general population, the panel recognized the uncertainty around the prognostic value of some WHO clinical stage 2 conditions, and data from modelling and observational studies indicating that more than 50% of HIV-infected patients with WHO clinical stage 2 have a CD4 count of ≤350 cells/mm3. The panel therefore recommended that all pregnant women with WHO clinical stages 1 and 2 should have access to CD4 testing in order to decide when to start treatment. What to start On the question of what to start, no GRADE evidence profiles were prepared as no RCTs were identified that compared the use of different ARV regimens in pregnant women. Cohort studies report a reduction of HIV transmission and death.(100) There is no evidence to suggest an increase in maternal serious adverse events and there are no studies specifically evaluating 15. Specific populations – when and what to start
- 50. 42 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach maternal response to ART. Registry data on the use of TDF in pregnancy show no signals to raise concern, and there is no evidence to suggest that TDF + 3TC (or FTC) is not an acceptable alternative to AZT + 3TC.(101,102) As discussed in the section on EFV, there is very low quality conflicting evidence on the risks of EFV causing neural tube defects, with the overall rates of birth defects reported in association with EFV, NVP and TDF similar to rates reported in congenital defects registries of general populations. However, data are currently insufficient to determine whether there is an increased risk of rare anomalies such as neural tube defects with first-trimester EFV exposure. The review of NVP safety in pregnant women with CD4 counts between 250 and 350 cells/mm3 did not confirm an increased risk of serious adverse events. However, while data from two prospective cohorts indicate no association between NVP and liver enzyme elevation, pregnancy itself was associated with an increased risk of any liver enzyme elevation and that this association was present, regardless of prior ART and NVP exposure history.(103) The panel concluded that the benefits of using NVP in pregnancy outweighed the risks. The panel was unable to conclude from the evidence reviewed whether there were benefits associated with the use of EFV compared to NVP in pregnant women after the first trimester and with higher or unknown CD4 cell counts, although more than half of the panel members preferred EFV in these situations. 15.2. Recommendations for women with prior exposure to antiretrovirals for PMTCT 1. Initiate a non-NNRTI-based ART in women who have received single-dose nevirapine (sdNVP) alone or in combination with other drugs without an NRTI tail within 12 months of initiating chronic ART. If an NNRTI-based regimen is started, perform viral load testing at 6 months and, if there are >5000 copies/ml, switch to a bPI-based regimen. 2. Initiate a standard NNRTI-based ART regimen in women who have received sdNVP alone or in combination with other drugs with an NRTI tail within 12 months of initiating chronic ART and perform viral load-testing at 6 months. If the viral load is >5000 copies/ml, changing to a bPI is recommended. 3. Initiate a standard NNRTI-based ART regimen in women who have received sdNVP (alone or in combination with other drugs) more than 12 months before starting therapy (with or without a NRTI tail) if possible. The viral load should be evaluated at 6 months and if it is >5000 copies/ml a change in the bPI-based regimen is required. Initiate a standard NNRTI regimen in women who have received ARV drugs such as AZT alone, without sdNVP, for PMTCT.
- 51. 43 Table 11. ART regimens recommended for women with prior exposure to PMTCT regimen Previous ARV exposure for PMTCT Recommendations for initiation of ART when needed for treatment of HIV for maternal health sdNVP1 (+/- antepartum AZT) with no AZT/3TC tail2 in last 12 months Initiate a non-NNRTI regimen PI preferred over 3 NRTI sdNVP (+/- antepartum AZT) with an AZT/3TC tail in last 12 months Initiate an NNRTI regimen If possible, check viral load3 at 6 months and if >5000 copies/ml, switch to second- line ART with PI sdNVP (+/- antepartum AZT) with or without an AZT/3TC tail over 12 months ago Initiate an NNRTI regimen If possible, check viral load3 at 6 months and if >5000 copies/ml, switch to second- line ART with PI Option A4 Antepartum AZT (from as early as 14 weeks of gestation) sdNVP at onset of labour* AZT + 3TC during labour and delivery* AZT + 3TC tail for 7 days postpartum* * sd-NVP and AZT + 3TC can be omitted if mother receives >4 weeks of AZT antepartum Initiate an NNRTI regimen If possible, check viral load3 at 6 months and if >5000 copies/ml, switch to second- line ART with PI If no sdNVP was given, start standard NNRTI (viral load does not need to be checked unless clinically indicated as no sdNVP received) All triple ARV regimens (including Option B), irrespective of duration of exposure and time since exposure Option B4 Triple ARV from 14 weeks gestation until after all exposure to breast milk has ended AZT + 3TC + LPV/r AZT + 3TC + ABC AZT + 3TC + EFV TDF + [3TC or FTC] + EFV Initiate standard NNRTI regimen If EFV-based triple ARV was used for prophylaxis and no tail (AZT + 3TC; or TDF + 3TC; or TDF + FTC) was given when triple ARV was discontinued after cessation of breastfeeding (or delivery if formula feeding), check viral load3 at 6 months and if >5000 copies/ml, switch to second-line ART with PI 1Single-dose nevirapine (sdNVP) is one 200-mg tablet of NVP. 2A tail is the provision of two NRTIs, typically AZT/3TC, for a minimum of 7 days following sdNVP or the cessation of any NNRTI-based regimen with the objective of minimizing NNRTI resistance. 3If VL is not available, continue NNRTI regimen and monitor clinically (and immunologically if available). 4Options A or B are viewed as equally effective for PMTCT in women who do not require therapy for their own health and are recommended options in the 2010 update of Use of antiretroviral drugs for treating pregnant women and preventing HIV infection in infants.
- 52. 44 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach Evidence The long half-life of NVP and its low genetic barrier to resistance means that detectable drug levels persist for 2−3 weeks in the presence of active viral replication following a single maternal dose. (104−106) EFV also has a long half-life, with detectable drug levels for more than 21 days following discontinuation.(107) This has clinical relevance in pregnancy when ARVs are provided solely for prophylaxis against perinatal transmission and discontinued after delivery or after breastfeeding. In a meta-analysis of 10 studies, the prevalence of NVP resistance 4 to 8 weeks following sdNVP was 35.7% and the prevalence of NVP resistance in infants who became infected despite prophylaxis was 52.6%.(108) In most women, resistant virus can no longer be detected 6 to 12 months after exposure. However, low levels of viral resistance can persist for longer periods and in some cases can remain present in latently infected cells.(109−111) Data suggest that women starting NNRTI-based therapy within 6−24 months of sdNVP exposure have higher rates of viral failure than those without sdNVP exposure. A definite relationship between time from sdNVP exposure to starting NNRTI-based therapy has been observed but varied between studies from 6 months to 24 months, with a definite improvement in response if >12 months since sdNVP exposure and start of therapy.(112−119) A tail regimen for a minimum of 7 days is recommended following sdNVP or if NNRTI-based triple therapy ART is used for the prevention of perinatal transmission and subsequently stopped. NNRTI resistance rates of 0% to 7% at 2 to 6 weeks postpartum have been reported with the use of various tail regimens. (120−125) 15.3. Recommendations for HIV/HBV coinfection 1. Start ART in all HIV/HBV-coinfected individuals who require treatment for their HBV infection, (chronic active hepatitis), irrespective of the CD4 cell count or the WHO clinical stage. (Strong recommendation, low quality of evidence) 2. Start TDF and 3TC (or FTC)-containing antiretroviral regimens in all HIV/HBV coinfected individuals needing treatment. (Strong recommendation, moderate quality of evidence) In developing these recommendations, the panel placed high value on promoting HBV diagnosis and more effective treatment of HIV/HBV coinfection. The systematic review of this topic did not find RCTs which addressed critical HIV outcomes (death, disease progression, serious adverse events) and the GRADE profile reported only on outcomes related to HBV (HBV viral load and HBV drug resistance). Liver biopsy and HBVDNA are not usually available in the large majority of resource-limited settings. A global definition of chronic active hepatitis for resource-limited settings based on clinical and available laboratory parameters is under discussion.
- 53. 45 When to start On the question of when to start ART in HIV/HBV coinfection, there are no RCTs comparing early versus late initiation of ART. However, observational data demonstrate that individuals with HIV/HBV coinfection have a threefold to sixfold increased risk of developing chronic HBV infection, an increased risk of fibrosis and cirrhosis and a 17-fold increased risk of death compared to HBV- infected individuals without HIV infection.(126,127) Similarly, observational data support a reduction in liver-related disease with earlier and HBV-active combination ART.(128) What to start On the question of what ART to start in HIV/HBV coinfection, there are data from one RCT supporting the use of at least two agents with activity against HBV (TDF plus 3TC or FTC) in terms of improved HBV viral load response and reduced development of HBV drug resistance. (129,130) 15.4. Recommendations for HIV/tuberculosis coinfection 1. Start ART in all HIV-infected individuals with active TB, irrespective of the CD4 cell count. (Strong recommendation, low quality of evidence) 2. Start TB treatment first, followed by ART as soon as possible afterwards (and within the first eight weeks). (Strong recommendation, moderate quality of evidence) 3. Use efavirenz (EFV) as the preferred NNRTI in patients starting ART while on TB treatment. (Strong recommendation, high quality of evidence) In making these recommendations, the panel placed high value on the reduction of early mortality from HIV/TB coinfection, the potential for reduction of TB transmission when all individuals with HIV are started on ART earlier, and improved morbidity/mortality, reduction of TB recurrence and improved management of TB for coinfected HIV/TB patients. When to start On the question of when to initiate ART in TB infection, one RCT (SAPIT study) provides moderate evidence for the early initiation of ART in terms of reduced all-cause mortality and improved TB outcomes.(131) Trial participants were grouped into “integrated” (immediate and end of TB drug initiation phases combined) and “sequential” treatment arms. Mortality was 55% lower in the integrated treatment arm (5.1/100 person-years) compared to the sequential treatment arm (11.6 per 100 person-years), which was terminated. The trial is continuing to examine the outcomes of starting ART immediately or starting at the completion of the initiation phase of TB treatment. Until further data are available, it is recommended that ART be initiated as soon as TB therapy is tolerated. Ideally, this may be as early as 2 weeks and not later than 8 weeks. There are limited data on the initiation of ART in patients with TB and CD4 counts of >350 cells/ mm3.
- 54. 46 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach Impact on TB transmission and incidence ART has been reported to reduce TB rates by up to 90% at the individual level and by approximately 60% at the population level, and to reduce TB recurrence rates by 50%.(13,132,133) Modelling suggests that the initiation of ART for all those with HIV/TB coinfection, if accompanied by high levels of coverage and ART adherence, reduces the number of TB cases, TB mortality rates and TB transmission at the population level.(134) What to start The recommendations from the 2006 ART guidelines are maintained. Specifically, EFV is recommended because of less interaction with rifampicin compared to NVP. For those HIV/TB coinfected individuals who are unable to tolerate EFV, an NVP-based regimen or a triple NNRTI (AZT + 3TC + ABC or AZT + 3TC + TDF) are alternative options. In the presence of rifampicin, no lead-in dose of NVP is required.(50,135−138). Similarly, if patients temporarily change from NVP to EFV because they need to take rifampicin-containing TB therapy and subsequently switch back to NVP on completion of TB treatment, no lead-in dosing of NVP is required.(60,61) 15.5. Rifabutin Background Drug interactions between rifampicin and boosted protease inhibitors (bPIs) prohibit the concomitant use of standard therapies for both HIV and TB. Rifampicin induces the cytochrome P450 enzyme system, lowering standard-dose bPI plasma concentrations by 75−90%. All bPIs (at standard doses) are contraindicated with rifampicin. LPV/r or SQV/r may be used with an adjusted, superboosted dose of RTV (LPV/r 400 mg/400 mg BID or SQV/r 400 mg/400 mg BID) or doubling the standard LPV/r daily dose (LPV/r 800 mg/200 mg BID) but this is associated with high levels of toxicity, and requires close clinical and laboratory monitoring. The recommendation to use LPV/r 800 mg/200 mg BID is based on low-quality evidence and is associated with a similar level of toxicity to LPV/r 400 mg/400 mg BID. However, this option may be more feasible in RLS, as LPV/r is widely available but RTV as a sole formulation is not.(139−142) There is no comparable recommendation for ATV/r, a WHO-preferred bPI (143). Unlike rifampicin, rifabutin has minimal effect on bPI plasma concentrations. Evidence In a systematic review conducted for this guideline update, ten clinical trials (five RCTs and five cohort studies) were identified, which assessed the efficacy and safety of rifabutin in TB infection with or without HIV infection. The five RCTs were included in a Cochrane review, which found no differences in TB cure or relapse rates between rifampicin and rifabutin.(28) In the five cohort studies, 313 individuals received rifabutin and ART, of whom 125 received a PI. Due to methodological issues, no rigorous efficacy assessment from these studies was possible, but there was no sign of rifabutin inferiority in comparison with rifampicin.
- 55. 47 Taken together, these studies report comparable safety and efficacy of rifabutin and rifampicin. However, evidence from RCTs comes largely from HIV-uninfected individuals, and data on the use of rifabutin with ART are limited to first-generation, usually unboosted, PIs. A further limitation is that the evidence in HIV-infected individuals receiving a bPI and rifabutin is based on only 125 patients. In addition, the clinical experience with rifabutin for TB disease in resource-limited settings is limited, especially in the context of the bPIs currently recommended by WHO. Clinical considerations Dosing The recommended dose of rifabutin in the presence of a bPI is 150 mg three times per week. (144) However, it should be noted that this dose has been reported to result in inadequate rifabutin levels and acquired rifabutin resistance.(145) Rifabutin is contraindicated if administered with the new NNRTI etravirine plus a bPI (37% reduction of etravirine levels). Adverse events The most common adverse events associated with rifabutin are neutropenia, leucopenia, elevations of hepatic enzymes, rash and upper gastrointestinal complaints, and, more rarely, uveitis. In the systematic review, discontinuation attributable to adverse events was uncommon. This review revealed one case report of uveitis in combination with a bPI.(146) Monitoring and programmatic implications This systematic review indicates that a bPI and rifabutin coadministration will not require intensive monitoring and can be used in primary care settings. However, the DOTS strategy promotes daily administration of TB therapy, preferably in FDCs.(147) Intermittent dosing of rifabutin will complicate the programmatic roll-out of TB therapy and precludes the development of rifabutin- containing FDCs. Further research is needed into the pharmacokinetics of rifabutin 75 mg once- daily in the presence of bPIs. Meanwhile, the ability to use standard bPI doses outweighs the inconvenience of intermittent dosing.
- 56. 48 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach 16.1. Recommendations 1. Where available, use viral load (VL) to confirm treatment failure. (Strong recommendation, low quality of evidence) 2. Where routinely available, use VL every 6 months to detect viral replication. (Conditional recommendation, low quality of evidence) 3. A persistent VL of >5000 copies/ml confirms treatment failure. (Conditional recommendation, low quality of evidence) 4. When VL is not available, use immunological criteria to confirm clinical failure. (Strong recommendation, moderate quality of evidence) In making these recommendations, the panel was concerned by the limitations of clinical and immunological monitoring for diagnosing treatment failure, and placed high value on avoiding premature or unnecessary switching to expensive second-line ART. The panel also valued the need to optimize the use of virological monitoring and ensure adherence. 16.2. Evidence A systematic review was conducted to assess different strategies for determining when to switch antiretroviral therapy regimens for first-line treatment failure among PLHIV in low-resource settings. Standard Cochrane systematic review methodology was employed. Outcomes of interest in order of priority were mortality, morbidity, viral load response, CD4 response and the development of antiretroviral resistance. 16.3. Summary of findings Based on the pooled analysis of the side-effects from two randomized trials (Home-based AIDS care [HBAC] and Development of antiretroviral therapy in Africa [DART]), clinical monitoring alone (compared to combined immunological and clinical monitoring or to combined virological, immunological and clinical monitoring) resulted in increases in mortality, disease progression and unnecessary switches, but there were no differences in serious adverse events.(148,149) However, in the HBAC trial, combined immunological and clinical monitoring was compared to combined virological, immunological and clinical monitoring, and there were no differences in mortality, disease progression, unnecessary switches or virological treatment failures.(148) Viral load measurement is considered a more sensitive indicator of treatment failure compared to clinical or immunological indicators. VL may be used in a targeted or routine strategy. The objective of the targeted strategy is to confirm suspected clinical or immunological failure, maximizing the clinical benefits of first-line therapy and reducing unnecessary switching to second-line therapy. Targeted VL may also be used earlier in the course of ART (within 4 to 6 months of ART initiation) to assess adherence and introduce an adherence intervention in at-risk patients before viral mutations start to accumulate.(150) 16. When to switch ART
- 57. 49 The objective of the routine VL strategy is to detect virological failure early, leading to adherence interventions or changes in therapy that will limit ongoing viral replications, reduce the risk of accumulation of resistance mutations and protect the drug susceptibility of second-line and subsequent therapies. While staying on a failing first-line therapy is associated with an increased mortality risk,(151) it is uncertain if VL monitoring, compared to clinical or immunological monitoring, affects critical outcomes. Immunological criteria appear to be more appropriate for ruling out than for ruling in virological failure.(152) Mathematical modelling that compared these three ART monitoring strategies did not find significantly different outcomes.(153) The use of virological monitoring strategies has been associated with earlier and more frequent switching to second-line regimens than the use of clinical/immunological monitoring strategies. However, data from ART programmes and global procurement systems also suggests that treatment switching has occurred at lower than expected rates in resource-limited settings. Low access to second-line drugs, difficulties in defining treatment failure and the limited availability of virological monitoring have been identified as important reasons for late switching. There is evidence to support a VL threshold of 5000−10 000 copies/ml to define failure in an adherent patient with no other reasons for an elevated VL (e.g. drug-drug interactions, poor absorption, intercurrent illness): this range of values is associated with higher rates of clinical progression and immunological deterioration in some cohort studies.(154,155) Immunological failure is not a good predictor of virological failure. Depending on the study, 8% to 40% of individuals who present with evidence of immunological failure have virological suppression and risk being unnecessarily switched to second-line ART.(156) While no consensus on ART monitoring and the diagnosis of failure was reached, the panel supported moves to reduce reliance on clinical failure definitions, expand the use immunological criteria and use viral load testing for confirmation of clinical/immunological failure in deciding when to switch to second-line therapy. 16.4. Benefits and risks Benefits More accurate assessment of treatment failure will reduce the delay in switching to second-line drugs. Targeted use of VL can limit unnecessary switching and routine use of VL can reduce the risk of resistance. While expensive, VL has the potential to save the cost of expensive second- line drugs by confirming that they are needed. Risks The optimum threshold for defining VL failure in a public health approach is still unknown, and there are limited data on the diagnostic accuracy of VL in resource-limited settings. There is a risk that resources used to expand laboratory capacity or conduct VL testing would divert funds away from expanding access to treatment.
- 58. 50 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach Acceptability and feasibility ART switching has occurred at lower than expected rates in resource-limited settings, and the limited use of virological monitoring has been identified as an important factor. Many countries are considering employing VL to optimize the use of expensive second-line drugs. The same rationale applies when third-line drugs are available. Physicians and PLHIV consider clinical and immunological monitoring insufficient to promote a timely switch and want VL monitoring. The initial and ongoing cost is high. The use of VL to confirm clinical-immunological switch (targeted approach) will cost less than the routine use of VL monitoring. Quality assurance programmes should be implemented at VL facilities irrespective of the VL strategy adopted. Central VL facilities with adequate specimen transportation from clinic to laboratory are feasible, as is point-of-care VL capacity in urban settings. Point-of-care VL capacity in rural settings is likely to remain unfeasible with current technologies. Feasibility was not systematically assessed, but targeted use of VL seemed more feasible to the panel than routine use. 16.5. Clinical considerations One of the critical decisions in ART management is when to switch from one regimen to another for treatment failure. The 2006 recommendations on Antiretroviral therapy for HIV infection in adults and adolescents recognized that definitions for treatment failure were not standardized and outlined a set of definitions for ART failure based on available evidence at that time. These remain basically unchanged except that the VL threshold for failure has changed from 10 000 copies/ml in 2006 recommendations to 5000 copies/ml in the current guidelines. An individual must be taking ART for at least 6 months before it can be determined that a regimen has failed. Table 12. ART switching criteria Failure Definition Comments Clinical failure New or recurrent WHO stage 4 condition Condition must be differentiated from immune reconstitution inflammatory syndrome (IRIS) Certain WHO clinical stage 3 conditions (e.g. pulmonary TB, severe bacterial infections), may be an indication of treatment failure
- 59. 51 Failure Definition Comments Immunological failure Fall of CD4 count to baseline (or below) OR 50% fall from on-treatment peak value OR Persistent CD4 levels below 100 cells/mm3 Without concomitant infection to cause transient CD4 cell decrease Virological failure Plasma viral load above 5000 copies/ml The optimal viral load threshold for defining virological failure has not been determined. Values of >5 000 copies/ml are associated with clinical progression and a decline in the CD4 cell count Fig. 1. Targeted viral load strategy for failure and switching Suspected clinical or immunological failure VL ≤ 5,000 copies/ml VL > 5,000 copies/ml Test viral load VL>5,000 copies/ml Adherence intervention Repeat VL Do not switch to second line Switch to second line
- 60. 52 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach Fig. 2. Routine viral load strategy for failure and switching NOTE: This algorithm also applies to the recommendation to check viral load 6 months after initiation of ART in women who have been exposed to sd-NVP for PMTCT. Routine Viral Load Testing (not a prerequisite for initiating ART) VL ≤ 5,000 copies/ml VL > 5,000 copies/ml Adherence intervention VL>5,000 copies/ml Repeat VL Do not switch to second line Switch to second line
- 61. 53 17.1. Recommendations 1. A boosted protease inhibitor (bPI) plus two nucleoside analogues (NRTIs) are recommended for second-line ART. (Strong recommendation, moderate quality of evidence) 2. ATV/r and LPV/r are the preferred bPIs for second-line ART. (Strong recommendation, moderate quality of evidence) 3. Simplification of second NRTI options is recommended. • If d4T or AZT has been used in first-line therapy, use TDF + (3TC or FTC) as the NRTI backbone in second- line therapy. • If TDF has been used in first-line therapy, use AZT + 3TC as the NRTI backbone in second- line theapy. (Strong recommendation, moderate quality of evidence) In making these recommendations, the panel placed high value on using simpler second-line regimens and the availability of heat-stable formulations and fixed-dose combinations. 17.2. Evidence A systematic review was conducted with the objective of assessing the optimum second-line ART regimen in PLHIV failing first-line therapy in resource-limited settings. Standard Cochrane systematic review methodology was employed. Outcomes of interest in order of priority were mortality, morbidity (combined disease progression and serious adverse events), viral load response, CD4 response and development of antiretroviral resistance. 17.3. Summary of findings Second-line NRTIs Despite a comprehensive search, few studies of relevance were identified. One study reported no difference in virological outcomes among those maintaining 3TC in second-line regimens compared to those who did not (low quality of evidence).(157) Observational data supported this finding.(158) Boosted PI comparisons bPIs provide most of the antiviral activity in second-line regimens. There is insufficient evidence on critical patient outcomes to distinguish between bPIs in the context of second-line therapy. Randomized trials comparing LPV/r with DRV/r, ATV/r or FPV/r in ART-naive patients showed non- inferiority at 48 weeks of all three bPIs (evidence of low to moderate quality).(159−163) DRV/r was superior to LPV/r at 96 weeks.(161) There is evidence of moderate quality that ATV/r is non-inferior to LPV/r (in combination with TDF and an optimized second NRTI) in treatment-experienced patients.(164) Non-serious adverse events varied by boosted PI and there were no significant differences in serious adverse events.(165,166). All unboosted PIs are considered inferior to bPIs. 17. Second-line regimens
- 62. 54 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach PI monotherapy On the question of whether PI monotherapy could be used as second-line ART, there is a moderate quality of evidence from a targeted review (as opposed to a formal systematic review) of nine RCTs and individual study reports showing less virological suppression and higher rates of viral rebound for PI monotherapy compared to standard triple ART regimens.(167−173) There were no other significant differences in the critical outcomes of mortality, disease progression or serious adverse events, or the important outcomes of immunological response and drug resistance (both very low to moderate quality evidence). Non-critical outcomes, such as non- serious adverse events and lipoatrophy, were not captured in the GRADE evidence profile. The panel concluded that an NRTI backbone should be maintained in a second-line bPI-containing regimen. 17.4. Benefits and risks Benefits These recommendations will facilitate the simplification of therapeutic options and drug procurement as the NRTIs recommended in second-line therapy are also used in first-line therapy (in different combinations), and should be purchased by all programmes. There is a potential for simplified drug regimens. Risks There may be confusion because AZT, TDF and 3TC, the only NRTIs recommended in second- line regimens, also are recommended in first-line regimens. Some countries have already chosen alternative bPIs (IDV/r, SQV/r, FPV/r) in preference to the recommended ones (ATV/r, LPV/r). 17.5. Acceptability and feasibility PLHIV want better second-line options with fewer side-effects. The preferred bPIs are available in most countries. Generic heat-stable LPV/r is on the market already. A generic heat-stable FDC of ATV/r (co-blister packed with TDF/3TC) is in development. Alternative bPIs (SQV, IDV, FPV and DRV) are not available as FDCs and are more expensive than the preferred options. Saquinavir has a high pill-burden, IDV has a high risk of toxicity and FPV is expensive. Clinicians may not be comfortable with not replacing both first-line NRTIs with two new NRTIs in the second-line regimen.
- 63. 55 17.6 Clinical considerations Table 13. Preferred second-line ART options Target population Preferred options Comments Adults and adolescents (including pregnant women) If d4T or AZT used in first-line therapy TDF + 3TC or FTC + ATV/r or LPVr NRTI sequencing based on availability of FDCs and potential for retained antiviral activity, considering early and late switch scenarios ATV/r and LPVr are comparable and available as heat-stable FDCs or co-package formulations If TDF used in first-line therapy AZT + 3TC + ATV/r or LPVr TB/HIV coinfection If rifabutin available Same regimens as recommended above for adults and adolescents No difference in efficacy between rifabutin and rifampicin Rifabutin has significantly less drug interaction with bPIs, permitting standard bPI dosing If rifabutin not available Same NRTI backbones as recommended for adults and adolescents plus LPVr or SQV/r with superboosted dosing of RTV (LPV/r 400 mg/400 mg twice daily or LPV/r 800 mg/200 mg twice daily or SQV/r 400 mg/400 mg twice daily) Rifampicin significantly reduces the levels of bPIs, limiting the effective options. Use of extra doses of ritonavir with selected bPIs (LPV and SQV) can overcome this effect but with increased rates of toxicity Hepatitis B coinfection AZT + TDF + 3TC or FTC + ATV/r or LPVr In case of ART failure, TDF + 3TC or FTC should be maintained for anti-HBV activity and the second-line regimen should include other drugs with anti-HIV activity
- 64. 56 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach 17.7. Selection of second-line NRTIs The rationale for the selection of the NRTIs in second-line therapy is to choose the most logical combination depending on what was used in the first-line regimen. Residual activity of first-line NRTIs (with the possible exception of 3TC and FTC) is more likely the earlier failure is detected and switching is implemented. Conversely, any new NRTIs may be compromised in the second- line regimen if there is late detection of failure and late switching. The recommended NRTI sequencing is based on likely resistance mutations and the potential for retained antiviral activity. There are two clinical scenarios: • early switching based on sensitive monitoring for failure, using viral load; • late switching based on insensitive monitoring, using clinical or immunological criteria for defining failure. If AZT + 3TC are used in the first-line regimen with sensitive monitoring and early switching, the NRTIs with most likely activity are TDF and ddI. In the scenario of insensitive monitoring and late switching, TDF and ddI activity are less likely. If TDF + 3TC are use in first-line therapy, with early or late switching, the NRTIs with remaining activity are AZT and d4T (both very likely). Retained activity of 3TC is likely in the early switching scenario and less likely in the case of late switching.(174) ABC and ddI are no longer recommended as preffered options in second-line regimens. The panel concluded that there was no specific advantage in using ABC or ddI and their use added complexity and cost, but new data will be generated from ongoing trials.(175) One study in the review reported no difference in viral suppression following mainly d4T-based first-line ART, with and without a ddI-containing NRTI backbone in an LPV/r-based second-line regimen.(176) Another study reported similar virological outcomes in individuals with and without the M184V mutation and taking a second-line regimen with or without ddI.(158) No studies reporting failure following a first-line ABC-containing (or TDF-containing) regimen were identified. 17.8. Maintaining 3TC in the second-line regimen There is uncertainty about whether 3TC should be added as a fourth drug in the NRTI component of second-line regimens if ddI or ABC are used as the backbone NRTIs. Only one RCT has been conducted to examine this issue; it found no significant difference in the reduction of HIVRNA in individuals who maintained 3TC in their second-line regimen compared to those who did not. (157) One observational study reported similar virological response among individuals with the M184V mutation (indicating resistance to 3TC and FTC) who subsequently took 3TC- or FTC- containing regimen compared to those who took a 3TC- or FTC-sparing regimen.(177)
- 65. 57 17.9. NRTIs for HIV/HBV coinfection In individuals with HIV/HBV coinfection who require treatment for their HBV infection and in whom TDF + (3TC or FTC) fail in the first-line regimen, these NRTIs should be continued in the second-line regimen for anti-HBV activity and to reduce the risk of hepatic flares, irrespective of the selected second-line regimen, which should be AZT + TDF + (3TC or FTC) + bPI. 17.10. Selection of boosted protease inhibitor The recommend bPIs are equivalent in terms of efficacy. In studies of populations with PI resistance, there is growing support for the use of once-daily bPI regimens in which the ritonavir component is only 100 mg per day. Such regimens have fewer gastrointestinal side-effects and less metabolic toxicity than regimens that use ritonavir boosting at a dose of 200 mg per day. (178,179) Large head-to-head trials have demonstrated non-inferiority or superiority of ATV/r compared with LPV/r, with less gastrointestinal and lipid toxicity.(159)
- 66. 58 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach 18.1. Recommendations 1. National programmes should develop policies for third-line therapy that consider funding, sustainability and the provision of equitable access to ART. (Conditional recommendation, low quality of evidence) 2. Third-line regimens should include new drugs likely to have anti-HIV activity, such as integrase inhibitors and second-generation NNRTIs and PIs. (Conditional recommendation, low quality of evidence) 3. Patients on a failing second-line regimen with no new ARV options should continue with a tolerated regimen. (Conditional recommendation, very low quality of evidence) The panel was concerned by unpublished cohort reports of high mortality among patients failing second-line therapy, but placed high value on balancing the need to develop policies for third- line therapy while expanding access to first-line therapy. It was recognized that many countries have financial constraints that might limit the adoption of third-line regimens. 18.2. Evidence A targeted literature review of relevant studies provides limited evidence to guide third-line strategies in resource-limited settings, with few studies of newer agents in these settings. Data from RCTs, predominantly in developed countries, are available for boosted darunavir (DRV/r), etravirine and raltegravir. Taken together, these data support the efficacy of these agents in highly ART-experienced patients. There was no uncertainty among the panel concerning the need for third-line regimens. However, there was uncertainty about how making third-line regimens available would affect the provision of first-line and second-line ART. There was also uncertainty about what third-line drugs should be provided, as many studies are still in progress. 18.3. Summary of findings The evidence is very limited, particularly in resource-limited settings. However, as access to monitoring improves and the scale-up of initial ART continues, demand for second-line and third-line regimens will increase. The criteria for diagnosing second-line failure are the same as those used for diagnosing first-line failure. In a pooled subgroup analysis, DRV/r plus an optimized background regimen (OBR) chosen by genotyping and phenotyping was shown to be superior to the control group (bPI plus OBR, where the bPI was selected by the investigator) in highly treatment-experienced individuals. (180,181) These studies were conducted in high- middle income countries (Argentina, Brazil) and some well-resourced settings. In a further analysis, DRV/r was well tolerated in treatment- experienced, HBV- or HCV-coinfected patients, with no differences in liver-related adverse events between DRV/r and the control bPI group.(182) In developed country settings, DRV/r has been reported to be cost-effective compared to LPV/r.(183) In individuals with limited treatment 18. Third-line regimens
- 67. 59 options, raltegravir (RAL) plus OBR provided better viral suppression than OBR alone for at least 48 weeks.(184,185) Similarly, etravirine (ETV) plus OBR provided better viral suppression and improved immunological response than OBR alone.(186) In patients with multidrug-resistant virus who have few remaining treatment options, the combination of RAL, ETV, and DRV/r was well tolerated, and was associated with a rate of virological suppression similar to that expected in treatment-naive patients.(187) 18.4. Benefits and risks Benefits Therapy with newer agents is associated with a reduction in clinical progression and immunological deterioration. DRV/r has a higher genetic barrier to resistance compared to early- generation PIs and is active against multidrug-resistant HIV isolates. While high-level resistance to ETV following NVP or EFV failure appears uncommon, low-level resistance is common. (188−190) Risks There are few studies of newer agents in third-line regimens in resource-limited settings.(191) Most studies have been conducted in well-resourced or high-income to middle-income countries, and have demonstrated benefit for non-critical outcomes (viral load suppression or immunological improvement). There is evidence from postmarketing reports of higher rates of hypersensitivity to ETV than previously reported.(192) Etravirine and raltegravir are not approved for use in individuals less than 16 years of age. There are limited data on the use of newer drugs in pregnancy, including very limited pharmacokinetic and safety data. 18.5. Acceptability and feasibility Physicians and PLHIV want a third-line regimen to be available. In studies conducted in well- resourced settings and in modelled cost-effectiveness analysis, DRV/r has been demonstrated to be cost-effective compared to other bPIs in heavily pretreated patients. The acquisition cost for ETV is one to two times higher than that of EFV and NVP. The acquisition cost of DRV and RAL has not been established in resource-limited settings but is expected to be high. The availability of these drugs in resource-limited settings now and in the near future is uncertain.
- 68. 60 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach 18.6. Clinical considerations Table 14. Toxicities of third-line ARVs Toxicities of third-line ARVs Darunavir (DRV) Skin rash (10%) – DRV has a sulfonamide moiety; Stevens- Johnson syndrome and erythrema multiforme have been reported Hepatotoxicity Diarrhoea, nausea Headache Hyperlipidaemia Transaminase elevation Hyperglycaemia Fat maldistribution Possible increased bleeding episodes in patients with haemophilia Ritonavir (RTV) (as pharmacokinetic booster) GI intolerance, nausea, vomiting, diarrhoea Paresthesias — circumoral and extremities Hyperlipidaemia (especially hypertriglyceridaemia) Hepatitis Asthenia Taste perversion Hyperglycaemia Fat maldistribution Possible increased bleeding episodes in patients with haemophilia Raltegravir (RAL) Nausea Headache Diarrhoea Pyrexia CPK elevation Etravirine (ETV) Rash (2 % discontinuation because of rash during clinical trials) Hypersensitivity reactions have been reported, characterized by rash, constitutional findings, and sometimes organ dysfunction, including hepatic failure Nausea
- 69. 61 19.1. Guiding principles 1. Countries should establish a package of care interventions, in addition to ART, to reduce HIV transmission, prevent illness and improve the quality of life. 2. A key component of the package of care interventions is the promotion of early HIV diagnosis and early assessment of ART eligibility by CD4 testing, in order to minimize late initiation of ART and maximize HIV prevention. 3. WHO continues to advocate for wider access to monitoring tools, including CD4 and viral load testing. 4. The package of care interventions should be aligned with the WHO Essential prevention and care interventions for adults and adolescents living with HIV in resource-limited settings.(193) Not all PLHIV are eligible for ART. However, it is imperative that as many PLHIV as possible enter care before they become ill with their first opportunistic infection (OI) or before they develop advanced immunosuppression (CD4 cell count <200 cells/mm3), which puts them at higher risk of developing opportunistic disease. Expanded access to HIV testing and counselling, especially provider-initiated but also client-initiated, is critical to identifying people who need to enter care. The pre-ART period in care provides a setting for interventions to prevent further transmission of HIV, to treat and prevent other illnesses, to prepare for the time when ART will be necessary and to maximize long-term retention in care. 19.2. Voluntary counselling and testing and provider-initiated testing and counselling Client-initiated voluntary counselling and testing (VCT) is the process whereby the client requests a test. However, attendance at any health facility offers an opportunity to integrate discussion of HIV and HIV testing into routine medical care through provider-initiated testing and counselling (PITC).(22) PITC facilitates early HIV diagnosis, partner diagnosis and enrolment into pre-ART care, and minimizes late initiation of ART. 19.3. Preventing further transmission of HIV From a public health perspective, PLHIV make up the most important group to address with HIV prevention strategies.(194) A change in the risk behaviour of a person with HIV has a greater impact on the transmission of HIV than the same behavioural change in a person without HIV. (195) Enrolment into care facilitates the identification of PLHIV with behavioural risk factors and interventions to reduce risk, and facilitates the identification of clinical risk factors, such as sexually transmitted infections and treatment, and interventions to reduce unplanned pregnancies and mother-to-child transmission of HIV.(196) 19. Package of care interventions
- 70. 62 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach Pre-ART care includes harm reduction for people who inject drugs (supportive environment, opioid substitution therapy and the provision of clean needles and syringes). This not only reduces HIV transmission but has the potential to stabilize the persons’ lifestyles by limiting active drug use in preparation for ART initiation. Positive prevention strategies, at group and individual levels, have demonstrated a reduction in HIV risk behaviours among people with HIV. They include support to improve the consistency of condom use, a reduction of needle-sharing and unprotected sex among people who inject drugs, and a reduction in the number of sexual partners.(197−199) 19.4. The Three I's for HIV/TB Among people living with HIV, TB is the most frequent life-threatening opportunistic infection and a leading cause of death. Pre-ART care provides a setting for implementation of the WHO Three I's strategy: isoniazid preventive treatment (IPT) where indicated, intensified case finding (ICF) for active TB, and TB infection control (IC) at all clinical encounters, which are key public health strategies to decrease the impact of TB among individuals and the community. The Three I's should be a central part of HIV care and treatment and are critical for the continued success of ART scale-up.(200) TB infection control is essential to keep vulnerable patients, health-care workers and their communities safe from becoming infected with TB.(200) Information about TB should be provided to all people with HIV. Counselling should include information about the risk of acquiring TB, strategies for reducing exposure, clinical manifestations of TB disease, and the risk of transmitting TB to others. 19.5. Cotrimoxazole prophylaxis Cotrimoxazole prophylaxis is recommended for all symptomatic individuals (WHO clinical stages 2, 3 or 4) including pregnant women. Where CD4 testing is available, cotrimoxazole prophylaxis is recommended for individuals with a CD4 cell count of <350 cells/mm3, particularly in resource-limited settings where bacterial infection and malaria are prevalent among PLHIV. If the main targets for cotrimoxazole prophylaxis are Pneumocystis jiroveci pneumonia and toxoplasmosis infection, a CD4 threshold of <200 cells/mm3 may be chosen. Data from an observational analysis in the DART trial showed that the use of cotrimoxazole prophylaxis reduced mortality by 50% in severely immune-suppressed HIV-infected adults initiating ART, with benefits continuing for at least 72 weeks. Furthermore, cotrimoxazole prophylaxis reduced malaria incidence in these patients.(201) 19.6. Sexually transmitted infections Pre-ART (and on-ART) care is an opportunity to provide comprehensive STI services, which should include correct diagnosis by syndrome or laboratory test, provision of effective treatment at the first encounter, notification and treatment of partners, reduction of further risk behaviour and transmission through education, counselling and the provision of condoms. Laboratory
- 71. 63 screening should include a serological test for syphilis, especially in pregnant women, and HIV testing for all individuals diagnosed with an STI.(196) 19.7. Treatment preparedness There is evidence that some PLHIV do not have access to accurate knowledge about HIV, the effectiveness of ART and the challenges of adherence.(202) In resource-limited settings, major factors contributing to good adherence are free ARVS, ease of use, and preparedness for use. (203) Modelling studies suggest that treatment readiness is associated with improved adherence once ART has commenced.(204) Enrolment into care before the time of initiation of ART provides an opportunity for PLHIV to learn, understand and prepare for successful lifelong ART. 19.8. Early initiation of ART Enrolment into pre-ART care is critical for the early initiation of ART, maximizing treatment response and minimizing treatment complication such as immune reconstitution inflammatory syndrome (IRIS).(205,206) In reality, most people do not receive any pre-ART care, presenting with advanced HIV disease, and this results in delayed initiation of ART. Mortality rates during the first year of ART are high (3−26%), most deaths occurring in the first few months, largely because of late presentation.(207) The fundamental need is for earlier HIV diagnosis, enrolment into care, ideally with CD4 count monitoring to determine eligibility for ART, and the initiation of ART before sickness occurs.(208) 19.9. ART as prevention Studies continue to support the benefits of ART for prevention.(209) There is evidence that individuals on fully suppressive ART who are adherent to the therapy are less likely to transmit HIV to sexual partners. Conversely, those with unrecognized HIV infection contribute significantly to onward sexual transmission. At an individual level, ART reduces viral load and infectiousness. (210) The use of ARV drugs has been proved to reduce MTCT of HIV.
- 72. 64 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach 20.1. Guiding principles 1. Laboratory monitoring is not a prerequisite for the initiation of ART. 2. CD4 and viral load testing are not essential for monitoring patients on ART. 3. Symptom-directed laboratory monitoring for safety and toxicity is recommended for those on ART. 4. If resources permit, use viral load in a targeted approach to confirm suspected treatment failure based on immunological and/or clinical criteria. 5. If resources permit, use viral load in a routine approach, measured every 6 months, with the objective of detecting failure earlier than would be the case if immunological and/or clinical criteria were used to define failure. Table 15. Laboratory monitoring before, during and after initiating ART Phase of HIV management Recommended test Desirable test At HIV diagnosis CD4 HBsAg Pre-ART CD4 At start of ART CD4 Hb for AZT1 Creatinine clearance for TDF2 ALT for NVP3 On ART CD4 Hb for AZT1 Creatinine clearance for TDF2 ALT for NVP3 At clinical failure CD4 Viral load At immunological failure Viral load Women exposed to PMCT interventions with sd-NVP with a tail within 12 months and without a tail within 6 months of initiating ART Viral load 6 months after initiation of ART 1 Recommended test in patients with high risk of adverse events associated with AZT (low CD4 or low BMI). 2 Recommended test in patients with high risk of adverse events associated with TDF (underlying renal disease, older age group, low BMI, diabetes, hypertension and concomitant use of a boosted PI or nephrotoxic drugs). 3 Recommended test in patients with high risk of adverse events associated with NVP (ART-naive HIV+ women with CD4 of >250 cells/mm3, HCV coinfection). Patients who are not yet eligible for ART should have CD4 count measurement every six months and more frequently as they approach the threshold to initiate ART. If feasible, HBsAg should be performed in order to identify people with HIV/HBV coinfection and who, therefore, should initiate TDF-containing ART. 20. Laboratory monitoring
- 73. 65 20.2. Laboratory monitoring on ART Two RCTs (DART and HBAC) and two observational studies have assessed laboratory monitoring strategies. The DART study compared a laboratory-driven monitoring strategy (CD4 cell count every 3 months) to a clinically-driven monitoring strategy.(211) There was a small but statistically significant difference in mortality and disease progression in favour of the laboratory strategy but only from the third year on ART. HBAC compared clinical monitoring alone to clinical monitoring and the addition of CD4 cell count or CD4 cell count and viral load, both performed every 3 months. In this study, clinical monitoring alone was associated with an increased rate of AIDS-defining events and a trend towards increased mortality. No additional benefit was seen from adding quarterly viral load measurements to CD4 cell count in the first 3 years of ART.(148) The two observational studies which compared immunological and clinical versus virological, immunological and clinical monitoring reported that, in programmes with virological, immunological and clinical monitoring a switch to second-line therapy occurred earlier, more frequently and at higher CD4 counts.(212) Three further monitoring trials, all of which are assessing viral load monitoring in different strategies, are progressing in Cameroon, Thailand, and Zambia.(213−215) For NNRTI-containing regimens, symptom-directed laboratory monitoring of liver enzymes is recommended. Symptom-directed monitoring means ordering tests only when the care provider recognizes signs and symptoms of potential ART-related toxicity. For women initiating NVP with a CD4 count of 250−350 cells/mm3, if feasible, it is recommended (but not required) to monitor hepatic enzymes at weeks 2, 4 and 12 after initiation. For AZT-containing regimens, haemoglobin (Hb) measurement is recommended before the initiation of AZT and then as indicated by signs/symptoms. Patients receiving AZT-containing regimens and with low body weight and/or low CD4 cell counts are at greater risk of anaemia. These patients should have routine Hb monitoring 1 month after initiating AZT and then at least every 3 months. AZT should not be given if Hb is <7 g/dl. For TDF-containing regimens, creatinine clearance calculation is recommended, if feasible, before initiation and every 6 months. The inability to perform creatinine clearance is not a barrier to TDF use. Creatinine clearance monitoring is recommended in those with underlying renal disease, of older age groups, and with low body weight or other renal risk factors such as diabetes or hypertension. There is evidence that individuals taking TDF and a PI/r may experience greater median decline in creatinine clearance than those taking TDF and an NNRTI-based regimen.(216) Creatinine clearance should be monitored more closely when TDF is used with a PI/r. For individuals with HIV/HBV or HIV/HCV coinfection it is recommended to monitor hepatic enzymes at weeks 4 and 12 following ART initiation if feasible.
- 74. 66 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach Table 16. Monitoring ART in those at higher risk of adverse events ARV drug Major toxicity High-risk situations* d4T Lipodystrophy Neuropathy Lactic acidosis Age >40 years CD4 count of <200 cells/mm3 BMI >25 (or body weight >75kg) Concomitant use with INH or ddI AZT Anaemia Neutropaenia CD4 count of <200 cells/mm3 BMI <18.5 (or body weight <50 kg) Anaemia at baseline TDF Renal dysfunction Underlying renal disease Age >40 years BMI <18.5 (or body weight <50 kg) Diabetes mellitus Hypertension Concomitant use of a bPI or nephrotoxic drugs EFV Teratogenicity first trimester of pregnancy (do not use EFV) Psychiatric illness Depression or psychiatric disease (previous or at baseline) NVP Hepatotoxicity HCV and HBV coinfection
- 75. 67 21.1. Special note on coinfection with HIV and hepatitis C Hepatitis C (HCV) coinfection is significantly associated with increased risk of death and advanced liver disease in HIV-positive individuals. HIV infection accelerates HCV-related disease progression and mortality (217−219) but the reciprocal effect of HCV on the rate of HIV disease progression remains difficult to quantify because of the heterogeneity of study results. A recent meta-analysis showed an increase in the overall risk of mortality but did not demonstrate an increased risk of AIDS-defining events among coinfected patients.(220) A major observational cohort study on the level of toxicities of specific ART regimens used for HIV/HCV coinfection did not find significant differences.(221) However, the systematic review on drug-drug interactions prepared for these guidelines found important pharmacological interactions between ribavirin and ABC, ATV, AZT, d4T and ddI that can increase the toxicity risk if these drugs are used concomitantly.(222−226) Many studies also suggest that the sustained viral response rates of HCV therapy in HIV- coinfected individuals are significantly lower than in HCV-monoinfected patients (227−230) but others have achieved higher rates in this population.(231) Considering the significant level of uncertainty on these topics and the importance of hepatitis C management in the context of HIV coinfection (an important gap highlighted by the guidelines panel group, particularly the representatives from the people living with HIV community), WHO is planning to revise the recommendations for the prevention and treatment of major HIV-related opportunistic infections and comorbidities, including hepatitis C. Furthermore, it is expected that the 2010 World Health Assembly will establish global policy recommendations for the management of viral hepatitis, which will increase support for an integrated approach to the prevention, treatment and care of HIV/HCV coinfection. Meanwhile, the initiation of ART in HIV/HCV coinfected people should follow the same principles and recommendations as for its initiation in HIV-monoinfected individuals. However, patients should be closely monitored because of the increased risk of drug toxicities and drug interactions between some ARVs and anti-HCV drugs. 21.2. Dosages of recommended antiretrovirals Generic name Dose Nucleoside reverse transcriptase inhibitors (NRTIs) Abacavir (ABC) 300 mg twice daily or 600 mg once daily Didanosine (ddI) 400 mg once daily (>60 kg) 250 mg once daily (≤60 kg) Emtricitabine (FTC) 200 mg once daily 21. Annexes
- 76. 68 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach Generic name Dose Lamivudine (3TC) 150 mg twice daily or 300 mg once daily Stavudine (d4T) 30 mg twice daily Zidovudine (AZT) 250−300 mg twice daily Nucleotide reverse transcriptase inhibitors (NtRTIs) Tenofovir 300 mg once daily1 Non-nucleoside reverse transcriptase inhibitors (NNRTIs) Efavirenz (EFV) 600 mg once daily Etravirine (ETV) 200 mg twice daily Nevirapine (NVP) 200 mg once daily for 14 days, followed by 200 mg twice daily2 Proteases inhibitors (PIs) Atazanavir + ritonavir (ATV/r) 300 mg + 100 mg once daily Darunavir + ritonavir (DRV/r) 600 mg + 100 mg twice daily Fos-amprenavir + ritonavir (FPV/r) 700 mg + 100 mg twice daily Indinavir + ritonavir (IDV/r) 800 mg + 100 mg twice daily Lopinavir/ritonavir (LPV/r) Fixed Dose Combination tablets (LPV 200 mg / RTV 50 mg) Two tablets (400 mg/200 mg) twice daily3 Considerations for individuals on TB therapy In the presence of rifabutin, no dose adjustment required In the presence of rifampicin; use ritonavir superboosting (LPV 400 mg + RTV 400 mg twice daily) or LPV 800 mg + RTV 200 mg twice daily ,with close clinical and hepatic enzyme monitoring
- 77. 69 Generic name Dose Saquinavir + ritonavir (SQV/r) 1000 mg + 100 mg twice daily Considerations for individuals on TB therapy In the presence of rifabutin, no dose adjustment required In the presence of rifampicin; use ritonavir superboosting (SQV 400 mg + RTV 400 mg twice daily) with close clinical and hepatic enzyme monitoring Integrase strand transfer inhibitors (INSTIs) Raltegravir (RAL) 400 mg twice daily 1 TDF dosage adjustment for individual with altered creatinine clearance can be considered (using Cockcroft-Gault formula). Creatinine clearance ≥50 ml/min, 300 mg once daily. Creatinine clearance 30−49 ml/min, 300 mg every 48 hours. Creatinine clearance ≥10−29ml/min (or dialysis), 300 mg once every 72−96 hours. Cockcroft-Gault formula: GFR = (140-age) x (Wt in kg) x (0.85 if female) / (72 x Cr) 2 In the presence of rifampicin, or when patients switch from EFV to NVP, no need for lead-in dose of NVP. 3 LPV/r can be administered as 4 tablets once daily ( i.e. LPV 800 mg + RTV 200 mg once daily) in patients with less than three LPV resistance-associated mutations on genotypic testing. Once-daily dosing is not recommended in pregnant women or patients with more than three LPV resistance-associated mutations. 21.3. Toxicities and recommended drug substitutions ARV drug Common associated toxicity Suggested substitute TDF Asthenia, headache, diarrhoea, nausea, vomiting, flatulence Renal insufficiency, Fanconi syndrome Osteomalacia Decrease in bone mineral density Severe acute exacerbation of hepatitis may occur in HBV- coinfected patients who discontinue TDF If used in first-line therapy AZT (or d4T if no other choice) If used in second-line therapy Within a public health approach, there is no option If patient has failed AZT/d4T in first-line therapy. If feasible, consider referral to a higher level of care where individualized therapy may be available
- 78. 70 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach ARV drug Common associated toxicity Suggested substitute AZT Bone marrow suppression: macrocytic anaemia or neutropaenia Gastrointestinal intolerance, headache, insomnia, asthenia Skin and nail pigmentation Lactic acidosis with hepatic steatosis If used in first-line therapy TDF (or d4T if no other choice) If used in second-line therapy d4T EFV Hypersensitivity reaction Stevens-Johnson syndrome Rash Hepatic toxicity Persistent and severe CNS toxicity (depression, confusion) Hyperlipidaemia Male gynaecomastia Potential teratogenicity (first trimester of pregnancy or women not using adequate contraception) NVP bPI if intolerant to both NNRTIs Triple NRTI if no other choice NVP Hypersensitivity reaction Stevens-Johnson syndrome Rash Hepatic toxicity Hyperlipidaemia EFV bPI if intolerant to both NNRTIs Triple NRTI if no other choice ATV/r Indirect hyperbilirubinaemia Clinical jaundice Prolonged PR interval — first degree symptomatic AV block in some patients Hyperglycaemia Fat maldistribution Possible increased bleeding episodes in individuals with haemophilia Nephrolithiasis LPV/r
- 79. 71 ARV drug Common associated toxicity Suggested substitute LPV/r GI intolerance, nausea, vomiting, diarrhoea Asthenia Hyperlipidaemia (especially hypertriglyceridaemia) Elevated serum transaminases Hyperglycaemia Fat maldistribution Possible increased bleeding episodes in patients with haemophilia PR interval prolongation QT interval prolongation and torsade de pointes ATV/r 21.4. ARV-related adverse events and recommendations Table 17. Symptom-directed toxicity management table Adverse events Major first- line ARVs Recommendations Acute pancreatitis d4T Discontinue ART. Give supportive treatment with laboratory monitoring. Resume ART with an NRTI with low pancreatic toxicity risk, such as AZT or TDF. Drug eruptions (mild to severe, including Stevens-Johnson syndrome or toxic epidermal necrolysis) NVP, EFV (less commonly) In mild cases, symptomatic care. EFV rash often stops spontaneously after 3−5 days without need to change ART. If moderate rash, non-progressing and without mucosal involvement or systemic signs, consider a single NNRTI substitution (i.e. from NVP to EFV). In moderate and severe cases, discontinue ART and give supportive treatment. After resolution, resume ART with a bPI-based regimen or triple NRTI if no other choice.
- 80. 72 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach Adverse events Major first- line ARVs Recommendations Dyslipidaemia All NRTIs (particularly d4T) EFV Consider replacing the suspected ARV Anaemia and neutropaenia AZT If severe (Hb <7.0 g/dl and/or ANC <750 cells/ mm3), replace with an ARV with minimal or no bone marrow toxicity (e.g. d4T or TDF) and consider blood transfusion Hepatitis All ARVs (particularly NVP) If ALT is at more than five times the basal level, discontinue ART and monitor. After resolution, restart ART, replacing the causative drug (e.g . EFV replaces NVP). Lactic acidosis All NRTIs (particularly d4T) Discontinue ART and give supportive treatment. After resolution, resume ART with TDF. Lipoatrophy and lipodystrophy All NRTIs (particularly d4T) Early replacement of the suspected ARV drug (e.g. d4T for TDF or AZT) Neuropsychiatric changes EFV Usually self-limited, without the need to discontinue ART. If intolerable to the patient, replace NVP with EFV or bPI. Single substitution recommended without cessation of ART. Renal toxicity (renal tubular dysfunction) TDF Consider substitution with AZT Peripheral neuropathy d4T Replacement of d4T with AZT, TDF. Symptomatic treatment (amitriptyline, vitamin B6).
- 81. 73 21.5. Diagnostic criteria for HIV-related clinical events Clinical event Clinical diagnosis Definitive diagnosis Clinical stage 1 Asymptomatic No HIV-related symptoms reported and no signs on examination Not applicable Persistent generalized lymphadenopathy Painless enlarged lymph nodes >1 cm, in two or more noncontiguous sites (excluding inguinal), in absence of known cause and persisting for 3 months or longer Histology Clinical stage 2 Moderate unexplained weight loss (under 10% of body weight) Reported unexplained weight loss. In pregnancy, failure to gain weight Documented weight loss (under 10% of body weight) Recurrent bacterial upper respiratory tract infections (current event plus one or more in last 6 months) Symptoms complex, e.g. unilateral face pain with nasal discharge (sinusitis), painful inflamed eardrum (otitis media), or tonsillopharyngitis without features of viral infection (e.g. coryza, cough) Laboratory studies if available, e.g. culture of suitable body fluid Herpes zoster Painful vesicular rash in dermatomal distribution of a nerve supply does not cross midline Clinical diagnosis Angular cheilitis Splits or cracks at the angle of the mouth not attributable to iron or vitamin deficiency, and usually responding to antifungal treatment Clinical diagnosis Recurrent oral ulcerations (two or more episodes in last 6 months) Aphthous ulceration, typically painful with a halo of inflammation and a yellow-grey pseudomembrane Clinical diagnosis
- 82. 74 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach Clinical event Clinical diagnosis Definitive diagnosis Papular pruritic eruption Papular pruritic lesions, often with marked postinflammatory pigmentation Clinical diagnosis Seborrhoeic dermatitis Itchy scaly skin condition, particularly affecting hairy areas (scalp, axillae, upper trunk and groin) Clinical diagnosis Fungal nail infections Paronychia (painful red and swollen nail bed) or onycholysis (separation of nail from nail bed) of the fingernails (white discolouration, especially involving proximal part of nail plate, with thickening and separation of nail from nail bed) Fungal culture of nail / nail plate material Clinical stage 3 Severe unexplained weight loss (more than 10% of body weight) Reported unexplained weight loss (over 10% of body weight) and visible thinning of face, waist and extremities with obvious wasting or body mass index below 18.5. In pregnancy, weight loss may be masked. Documented loss of more than 10% of body weight Unexplained chronic diarrhoea for longer than 1 month Chronic diarrhoea (loose or watery stools three or more times daily) reported for longer than 1 month Not required but confirmed if three or more stools observed and documented as unformed, and two or more stool tests reveal no pathogens Unexplained persistent fever (intermittent or constant and lasting for longer than 1 month) Reports of fever or night sweats for more than 1 month, either intermittent or constant with reported lack of response to antibiotics or antimalarials, without other obvious foci of disease reported or found on examination. Malaria must be excluded in malarious areas. Documented fever exceeding 37.6 oC with negative blood culture, negative Ziehl-Nielsen stain, negative malaria slide, normal or unchanged chest X-ray and no other obvious focus of infection
- 83. 75 Clinical event Clinical diagnosis Definitive diagnosis Oral candidiasis Persistent or recurring creamy white curd-like plaques which can be scraped off (pseudomembranous), or red patches on tongue, palate or lining of mouth, usually painful or tender (erythematous form) Clinical diagnosis Oral hairy leukoplakia Fine white small linear or corrugated lesions on lateral borders of the tongue, which do not scrape off Clinical diagnosis Pulmonary TB Chronic symptoms (lasting at least 2 to 3 weeks): cough, haemoptysis, shortness of breath, chest pain, weight loss, fever, night sweats, plus EITHER positive sputum smear OR negative sputum smear AND compatible chest radiograph (including but not restricted to upper lobe infiltrates, cavitation, pulmonary fibrosis and shrinkage). No evidence of extrapulmonary disease. Isolation of M. tuberculosis on sputum culture or histology of lung biopsy (together with compatible symptoms) Severe bacterial infection (e.g. pneumonia, meningitis, empyema, pyomyositis, bone or joint infection, bacteraemia, severe pelvic inflammatory disease) Fever accompanied by specific symptoms or signs that localize infection, and response to appropriate antibiotic Isolation of bacteria from appropriate clinical specimens (usually sterile sites) Acute necrotizing ulcerative stomatitis, gingivitis or periodontitis Severe pain, ulcerated gingival papillae, loosening of teeth, spontaneous bleeding, bad odour, rapid loss of bone and/or soft tissue Clinical diagnosis
- 84. 76 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach Clinical event Clinical diagnosis Definitive diagnosis Unexplained anaemia (below 8g/dl), neutropenia (below 0.5 x 109/l) and/or chronic (more than 1 month) thrombocytopenia (under 50 x 109/l) No presumptive clinical diagnosis Diagnosed on laboratory testing and not explained by other non-HIV conditions. Not responding to standard therapy with haematinics, antimalarials or anthelmintics as outlined in relevant national treatment guidelines, WHO IMCI guidelines or other relevant guidelines. Clinical stage 4 HIV wasting syndrome Reported unexplained weight loss (over 10% of body weight) with obvious wasting or body mass index below 18.5, plus EITHER unexplained chronic diarrhoea (loose or watery stools three or more times daily) reported for longer than 1 month OR reports of fever or night sweats for more than 1 month without other cause and lack of response to antibiotics or antimalarials. Malaria must be excluded in malarious areas. Documented weight loss (over 10% of body weight) plus two or more unformed stools negative for pathogens OR documented temperature exceeding 37.6 oC with no other cause of disease, negative blood culture, negative malaria slide and normal or unchanged CXR Pneumocystis pneumonia Dyspnoea on exertion or nonproductive cough of recent onset (within the past 3 months), tachypnoea and fever; AND CXR evidence of diffuse bilateral interstitial infiltrates, AND no evidence of bacterial pneumonia. Bilateral crepitations on auscultation with or without reduced air entry. Cytology or immunofluorescent microscopy of induced sputum or bronchoalveolar lavage (BAL), or histology of lung tissue
- 85. 77 Clinical event Clinical diagnosis Definitive diagnosis Recurrent bacterial pneumonia (this episode plus one or more episodes in last 6 months) Current episode plus one or more episodes in last 6 months. Acute onset (under 2 weeks) of symptoms (e.g. fever, cough, dyspnoea, and chest pain) PLUS new consolidation on clinical examination or CXR. Response to antibiotics. Positive culture or antigen test of a compatible organism Chronic herpes simplex virus (HSV) infection (orolabial, genital or anorectal) of more than 1 month, or visceral at any site or any duration Painful, progressive anogenital or orolabial ulceration; lesions caused by recurrent HSV infection and reported for more than one month. History of previous episodes. Visceral HSV requires definitive diagnosis. Positive culture or DNA (by PCR) of HSV or compatible cytology/histology Oesophageal candidiasis Recent onset of retrosternal pain or difficulty in swallowing (food and fluids) together with oral candidiasis Macroscopic appearance at endoscopy or bronchoscopy, or by microscopy/histology Extrapulmonary TB Systemic illness (e.g. fever, night sweats, weakness and weight loss). Other evidence for extrapulmonary or disseminated TB varies by site: pleural, pericardial, peritoneal involvement, meningitis, mediastinal or abdominal lymphadenopathy, osteitis. Miliary TB: diffuse uniformly distributed small miliary shadows or micronodules on CXR. Discrete cervical lymph node M. tuberculosis infection is usually considered a less severe form of extrapulmonary tuberculosis. M. tuberculosis isolation or compatible histology from appropriate site, together with compatible symptoms/ signs (if culture/histology is from respiratory specimen there must be other evidence of extrapulmonary disease)
- 86. 78 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach Clinical event Clinical diagnosis Definitive diagnosis Kaposi sarcoma Typical appearance in skin or oropharynx of persistent, initially flat patches with a pink or blood-bruise colour, skin lesions that usually develop into violaceous plaques or nodules Macroscopic appearance at endoscopy or bronchoscopy, or by histology Cytomegalovirus disease (retinitis or infection of other organs, excluding liver, spleen and lymph nodes) Retinitis only: may be diagnosed by experienced clinicians. Typical eye lesions on fundoscopic examination: discrete patches of retinal whitening with distinct borders, spreading centrifugally, often following blood vessels, associated with retinal vasculitis, haemorrhage and necrosis. Compatible histology or CMV demonstrated in CSF by culture or DNA (by PCR) CNS toxoplasmosis Recent onset of a focal neurological abnormality or reduced level of consciousness AND response within 10 days to specific therapy. Positive serum toxoplasma antibody AND (if available) single/multiple intracranial mass lesion on neuroimaging (CT or MRI) HIV encephalopathy Clinical finding of disabling cognitive and/or motor dysfunction interfering with activities of daily living, progressing over weeks or months in the absence of a concurrent illness or condition, other than HIV infection, which might explain the findings Diagnosis of exclusion, and, if available, neuroimaging (CT or MRI) Extrapulmonary cryptococcosis (including meningitis) Meningitis: usually subacute, fever with increasingly severe headache, meningism, confusion, behavioural changes that respond to cryptococcal therapy Isolation of Cryptococcus neoformans from extrapulmonary site or positive cryptococcal antigen test (CRAG) on CSF/blood
- 87. 79 Clinical event Clinical diagnosis Definitive diagnosis Disseminated non- tuberculous mycobacteria infection No presumptive clinical diagnosis Diagnosed by finding atypical mycobacterial species from stool, blood, body fluid or other body tissue, excluding lung Progressive multifocal leukoencephalopathy (PML) No presumptive clinical diagnosis Progressive neurological disorder (cognitive dysfunction, gait/speech disorder, visual loss, limb weakness and cranial nerve palsies) together with hypodense white matter lesions on neuroimaging or positive polyomavirus JC (JCV) PCR on CSF Cryptosporidiosis (with diarrhoea lasting more than 1 month) No presumptive clinical diagnosis Cysts identified on modified ZN microscopic examination of unformed stool Chronic isosporiasis No presumptive clinical diagnosis Identification of Isospora Disseminated mycosis (coccidiomycosis, histoplasmosis) No presumptive clinical diagnosis Histology, antigen detection or culture from clinical specimen or blood culture Recurrent septicemia (including non-typhoid salmonella) No presumptive clinical diagnosis Blood culture Lymphoma (cerebral or B cell non-Hodgkin) or other solid HIV- associated tumours No presumptive clinical diagnosis Histology of relevant specimen or, for CNS tumours, neuroimaging techniques Invasive cervical carcinoma No presumptive clinical diagnosis Histology or cytology
- 88. 80 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach Clinical event Clinical diagnosis Definitive diagnosis Atypical disseminated leishmaniasis No presumptive clinical diagnosis Histology (amastigotes visualized) or culture from any appropriate clinical specimen HIV-associated nephropathy No presumptive clinical diagnosis Renal biopsy HIV-associated cardiomyopathy No presumptive clinical diagnosis Cardiomegaly and evidence of poor left ventricular function confirmed by echocardiography Source: Revised WHO Clinical staging and immunological classification of HIV and case definition of HIV for surveillance. 2006.
- 90. 82 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach Chemistries Mild Grade1 Moderate Grade2 Severe Grade3 Potentially life-threatening Grade4 Hyperbilirubinaemia>1.0−1.5xULN>1.5−2.5xULN>2.5−5xULN>5xULN Glucose(fasting)110−125mg/dl126−250mg/dl251−500mg/dl>500mg/dl Hypoglycaemia55−64mg/dlOR 3.01−3.55mmol/l 40−54mg/dlOR 2.19−3.00mmol/l 30−39mg/dlOR 1.67−2.18mmol/l <30mg/dlOR <1.67mmol/l Hyperglycaemia (nonfastingandno priordiabetes) 116−160mg/dlOR 6.44−8.90mmol/l 161−250mg/dlOR 8.91−13.88mmol/l 251−500mg/dlOR 13.89−27.76 mmol/l >500mg/dlOR >27.76mmol/l Triglycerides−400−750mg/dlOR 4.52−8.47mmol/l 751−1200mg/dl OR 8.48−13.55mmol/l >1200mg/dlOR >13.55mmol/l Creatinine>1.0−1.5xULN>1.5−3.0xULN>3.0−6.0xULN>6.0xULN AST(SGOT)1.25−2.5xULN>2.5−5.0xULN>5.0−10.0xULN>10.0xULN ALT(SGPT)1.25−2.5xULN>2.5−5.0xULN>5.0−10.0xULN>10.0xULN GGT1.25−2.5xULN>2.5−5.0xULN>5.0−10.0xULN>10.0xULN Alkaline phosphatase 1.25−2.5xULN>2.5−5.0xULN>5.0−10.0xULN>10.0xULN Bilirubin1.1−1.5XULN1.6−2.5xULN2.6−5.0xULN>5xULN Amylase>1.0−1.5xULN>1.5−2.0xULN>2.0−5.0xULN>5.0xULN Pancreaticamylase>1.0−1.5xULN>1.5−2.0xULN>2.0−5.0xULN>5.0xULN
- 92. 84 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach Respiratory Mild Grade1 Moderate Grade2 Severe Grade3 Potentially life-threatening Grade4 DyspnoeaDyspnoeaon exertion Dyspnoeawith normalactivity DyspnoeaatrestDyspnoearequiring O2therapy Urinalysis Mild Grade1 Moderate Grade2 Severe Grade3 Potentially life-threatening Grade4 Proteinuria Spoturine1+2+or3+4+Nephrotic syndrome 24-hoururine200mgto1gloss/ dayOR<0.3%OR <3g/l 1gto2gloss/ dayOR0.3%to 1.0%OR3gto10 g/l 2gto3.5gloss/dayOR>1.0%OR >10g/l Nephrotic syndromeOR >3.5gloss/day GrosshaematuriaMicroscopiconlyGross,noclotsGrossplusclotsObstructive Miscellaneous Mild Grade1 Moderate Grade2 Severe Grade3 Potentially life-threatening Grade4 Fever(oral,>12 hours) 37.7−38.50COR 100.0−101.50F 38.6−39.50COR 101.6−102.90F 39.6−40.50COR 103−1050F >40.50COR >1050Ffor≥12 continuoushours
- 94. 86 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach 21.7. Prevention and Assessment of HIV Drug Resistance The emergence of HIV drug resistance (HIVDR) is of increasing concern in countries where ART and ARV prophylaxis is widely used, and represents a potential impediment to the achievement of long-term success in treatment outcomes. The rapid or uncontrolled emergence of HIVDR could lead to an increase in therapeutic failures, transmission of resistant virus, and a decrease in therapeutic options, treatment programme effectiveness and survival. Implementing programme elements that minimize the emergence of HIVDR, including optimizing access to ART, supporting appropriate ART prescribing and adherence, and ensuring adequate and continuous drug supplies, is essential for preserving the efficacy of the limited number of ARV drugs available in many countries.i Transmission of resistant virus is minimized through support for prevention programmes for HIV positive individuals. To guide these interventions, WHO, together with its partners in The Global HIV Drug Resistance Network (HIVResNet), developed and encourages countries to adopt an HIVDR prevention and assessment strategy. The goal of the strategy, coordinated at country level by a national HIVDR working group, is to support development of evidence to inform programme actions that maintain the effectiveness of ART regimens and limit HIVDR transmission. The elements, which comprise an important public health tool to support national, regional and global ART scale-up efforts, include: Regular monitoring of key early warning indicators in ART sites that may be programmatically improved to minimize the emergence of HIVDR; Monitoring surveys to assess the emergence of HIVDR and associated factors in cohort(s) of treated patients 12 months after ART initiation in sentinel ART sites; and Surveillance for transmitted drug-resistant HIV-1 among individuals newly infected. Further information on and resources to support the WHO HIVDR prevention and assessment strategy are available at http://www.who.int/hiv/drugresistance/. i Note that WHO does not recommend routine HIV drug resistance testing for individual patient management in settings where other basic laboratory measurements such as CD4 and HIV VL are not yet available.
- 95. 87 21.8. Special Note on Antiretroviral Pharmacovigilance Background Pharmacovigilance is the science and activities relating to the detection, assessment, understanding and prevention of adverse effects or any other possible drug-related problems.ii It incorporates and provides training in the identification of adverse reactions, data collection, processing, analysis and reporting. Pharmacovigilance is a key component of comprehensive patient care and the safe use of medicines. Adverse events and severe adverse events, both pre and post marketing, have been reported with all antiretrovirals. Not monitoring, understanding and managing these events can result in poor adherence, treatment failure and reduce confidence in ART by both PLHIV and care providers. Objectives of pharmacovigilance The main objectives of pharmacovigilance in antiretroviral programs are to maximize patient safety and the outcomes of public health programs, identify early warning signs (signals) of adverse reactions to drugs used in the management of HIV infection, monitor the safety of antiretrovirals in specific groups including pregnant women and in children, identify drug-drug interactions and quantify the rates of these events and report them to health authorities/ clinicians. Pharmacovigilance programs also provide methodological training and address issues related to unregulated prescribing, drug quality control and counterfeit drugs. Pharmacovigilance in resource limited settings In resource limited settings, antiretroviral pharmacovigilance is poorly developed but is critical because of factors unique to these settings. There has been rapid scale-up of largely generic antiretroviral therapy drug combinations not commonly used in well-resource settings. Pharmacovigilance is required not only for chronic antiretroviral therapy but also for the antiretrovirals used for the prevention of mother to child transmission of HIV. There are distinct co-comorbidities (tuberculosis, malaria) and drug-drug interactions. Methodology There are two main methods of monitoring, cohort event monitoring (CEM) and spontaneous reporting. A third method is consumer reporting, whereby a report of a suspected adverse drug reaction is initiated by the drug consumer. In spontaneous reporting systems, suspected adverse drug events are voluntarily submitted by health professionals and pharmaceutical manufacturers to the national regulatory authority. Spontaneous reporting is the most common form of pharmacovigilance and is the core activity of national pharmacovigilance centres participating in the WHO international drug monitoring program. It requires fewer human and financial resources than CEM, and is likely to be the method used in most resource limited settings in the foreseeable future. The system has limitations. The success or failure of a spontaneous reporting system depends on the active participation of reporters. Under reporting is common in all counties, irrespective of their ii The safety of medicines in public health programmes: Pharmacovigilance an essential tool (WHO, 2006).
- 96. 88 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach resources. Without information on utilization and on the extent of consumption, spontaneous reports do not make it possible to determine the frequency of an adverse drug reaction attributable to a product, or its safety in relation to a comparator.iii CEM is a prospective observational cohort study of adverse events associated with one or more medicines. In CEM, all adverse events occurring in a patient taking antiretroviral are collected irrespective of causality or relationship the antiretrovirals. Advantages of CEM (over spontaneous reporting) include the ability to produce rates, rapid results, early detection of signals, fewer missing data and less reporting bias. However, CEM is requires more resources than spontaneous reporting. WHO and partners are preparing a toolkit for countries wishing incorporate pharmacovigilance into their antiretroviral programs. In the mean time, the following resources are available: • Pharmacovigilance for antiretrovirals home page http://www.who.int/hiv/topics/pharmacovigilance/en/index.html • A practical handbook on the pharmacovigilance of antiretroviral medicines (WHO 2009) http://www.who.int/hiv/topics/pharmacovigilance/arv_pharmacovigilance_handbook.pdf • Pharmacovigilance for antiretroviral in resource limited settings (WHO 2007) http://www.who.int/medicines/publications/PhV_for_antiretrovirals.pdf • The safety of medicines in public health programmes: Pharmacovigilance an essential tool (WHO 2006) www.who.int/medicines/areas/quality_safety/safety_efficacy/Pharmacovigilance_B.pdf • The importance of pharmacovigilance: Safety Monitoring of medicinal products http://apps.who.int/medicinedocs/pdf/s4893e/s4893e.pdf iii Meyboom RHB, Egberts ACG, Gribnau FWJ, Hekster YA. Pharmacovigilance in perspective. Drug Safety 1999; 21(6): 429-447.
- 97. 89 21.9 GRADE evidence tables The following tables present profiles of the evidence considered for the recommendations made in these guidelines. For further information on the methodology of the GRADE process see The Conchrane handbook for systematic reviews of interventions, available at http://cochrane-handbook.org.
- 98. 90 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach WhentostartART Authors: NandiLSiegfried,OlolakenUthman,GeorgeWRutherford Date: 11Sep2009 Question: EarlyARTversusstandardordeferredART(CD4≤200orCD4≤250cells/µl)forasymptomatic,HIV-infected, treatment-naiveadults. Bibliography: SiegfriedNL,UthmanO,RutherfordGW.Optimaltimeofinitiationforasymptomatic,HIV-infected,treatment-naive adults.CochraneDatabase ofSystematicReviews. Qualityassessment Summaryoffindings Importance No.ofpatientsEffect QualityNo.of studies DesignLimitations Inconsis- tency Indirect- ness Impreci- sion Other consider- ations EarlyART versus standardor deferred ART(CD4 ≤200or CD4≤250 ells/µl) Control Relative (95%CI) Absolute Death 2Random- izedtrials Noserious limitations1 Noserious inconsis- tency Noserious indirectness Noserious imprecision Reporting bias2 6/539(1.1%) 24/526 (4.6%) RR0.26 (0.11to 0.62) 34fewerper 1000(from 17fewerto 41fewer) ⊕⊕⊕O MODERATE CRITICAL Tuberculosis 2Random- izedtrials Noserious limitations1 Noserious inconsis- tency Noserious indirectness Noserious imprecision Reporting bias219/539 (3.5%) 36/526 (6.8%) RR0.54 (0.26to 1.12) 31fewerper 1000(from 51fewerto 8more) ⊕⊕⊕O MODERATE CRITICAL
- 100. 92 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach WhatARTtostart Authors: GeorgeRutherford,AlicenSpauldin Date: 8Oct2009 Question: ShouldEFVvsNVPbeusedforinitialART?(Randomizedclinicaltrials) Settings: Multiplelocations Bibliography: 1.AyalaGaytanJJ,delaGarzaERZ,GarciaMC,ChavezSBV.Nevirapineorefavirenzincombinationwithtwo nucleosideanaloguesinHIVinfectedantiretroviralnaivepatients.MedInternMex2004;20:24.2.ManosuthiW, SungkanuparphS,TantanathipP,LueangniyomkulA,MankatithamW,PrasithsirskulW,BuraptarawongS,Thongyen S,LikanonsakulS,ThawornwaU,PrommoolV,KuxrungthamK,2NRStudyTeam.Arandomizedtrialcomparing plasmadrugconcentrationsandefficaciesbetween2nonnucleosidereverse-transcriptaseinhibitor-basedregimens inHIV-infectedpatientsreceivingrifampicin:theN2RStudy.ClinInfectDis2009;48:1752-9.3.NúñezM,SorianoV, Martín-CarboneroL,BarriosA,BarreiroP,BlancoF,García-BenayasT,González-LahozJ.SENC(SpanishEfavirenz vs.NevirapineComparison)trial:arandomized,open-labelstudyinHIV-infectednaiveindividuals.HIVClinTrials 2002;3:186-94.4.SowPG,BadianeM,DialloPD,LoI,NdiayeB,GayeAM.Efficacyandsafetyof lamivudine+zidovudine+efavirenzandlamivudine+zidovudine+névirapineintreatmentHIV1infectedpatients.A rétrospectivecrossstudyanalysis[AbstractCDB0584].XVIInternationalAIDSConference,Toronto,Canada,13−18 August2006.5.vandenBerg-WolfM,HullsiekKH,PengG,KozalMJ,NovakRM,ChenL,CraneLR,MacarthurRD; CPCRA058StudyTeam,theTerryBeirnCommunityProgramsforClinicalResearchonAIDS(CPCRA),andThe InternationalNetworkforStrategicInitiativeinGlobalHIVTrials(INSIGHT).Virologic,immunologic,clinical,safety, andresistanceoutcomesfromalong-termcomparisonofefavirenz-basedversusnevirapine-basedantiretroviral regimensasinitialtherapyinHIV-1-infectedpersons.HIVClinTrials2008;9:324-36.6.vanLethF,KappelhoffBS, JohnsonD,LossoMH,Boron-KaczmarskaA,SaagMS,HallDB,LeithJ,HuitemaAD,WitFW,BeljnenJH,LangeJM; 2NNStudyGroup.Pharmacokineticparametersofnevirapineandefavirenzinrelationtoantiretroviralefficacy.AIDS ResHumRetroviruses2006;22:232-39.
- 102. 94 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach Immunologicalresponse(follow-up4studiesat48weeks,1studyat65months,1studyat6months;betterindicatedbyhighervalues) 5Random- izedtrials Noserious limitations1 Noserious inconsis- tency Noserious indirect- ness2 Serious5None4 643639- MD3.95 higher (11.58lower to19.48 higher) ⊕⊕⊕O MODER- ATE IMPORTANT Drugresistance(follow-upmedian65months) 1Random- izedtrials Serious1,6Noserious inconsis- tency Noserious indirect- ness2 Serious3None4 32/111 (28.8%) 49/117 (41.9%) RR0.69 (0.48to 0.99) 130fewer per1000 (from4 fewerto 218fewer) ⊕⊕OO LOW IMPORTANT SexualtransmissionofHIVnotreported 0-----None0/0(0%)0/0(0%)-- 1 4of6studieswereopen-label;1oftheremainingstudiesdidnotprovidesufficientinformationonblinding(Sow)andtheotherwasblinded(vanden Berg-Wolf)butstudieswerenotdowngradedbasedonthesefacts. 2 1study(vandenBergetal.)lookedatmultipleindirectcomparisons.Also,only1of6studieswasonlyconductedinadevelopedcountrysetting (Manosuthi). 3 Numberofevents<300and/orconfidenceintervalsincludepotentialharmandbenefit. 4 1of6studieswereindustry-funded(vanLethetal.),while1of6studieshadafundingsourcethatwasunclear. 5 NoneoftheincludedstudiesprovidedstandarddeviationsforthemeanoutcomesothesameestimatedSDvaluewasusedforallstudies. 6 Only1studyreportedondrugresistance(vandenBerg-Wolfetal.),suggestingselectivereporting.
- 104. 96 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach L,QuilletC,FontanetA.Responsetohighlyactiveantiretroviraltherapyamongseverelyimmuno-compromisedHIV-infectedpatients inCambodia.AIDS2007;21:351-9.15.ManosuthiW,SungkanuparphS,VibhagoolA,RattanasiriS,ThakkinstianA.Nevirapine-versus efavirenz-basedhighlyactiveantiretroviraltherapyregimensinantiretroviral-naivepatientswithadvancedHIVinfection.HIVMed 2004;5:105-9.16.ManosuthiW,MankatithamW,LueangniyomkulA,ChimsuntornS,SungkanuparphS.Standard-doseefavirenzvs. standard-dosenevirapineinantiretroviralregimensamongHIV-1andtuberculosisco-infectedpatientswhoreceivedrifampicin.HIV Med2008;9:294-99.17.Martín-CarboneroL,NúñezM,González-LahozJ,SorianoV.Incidenceofliverinjuryafterbeginning antiretroviraltherapywithefavirenzornevirapine.HIVClinTrials2003;4:115-20.18.MatthewsGV,SabinCA,MandaliaS,LampeF, PhillipsAN,NelsonMR,BowerM,JohnsonMA,GazzardBG.Virologicalsuppressionat6monthsisrelatedtochoiceofinitialregimen inantiretroviral-naivepatients:acohortstudy.AIDS2002;16:53–61.19.NachegaJB,HislopM,DowdyDW,GallantJE,ChaissonRE, RegensbergL,MaartensG.Efavirenzversusnevirapine-basedinitialtreatmentofHIVinfection:clinicalandvirologicaloutcomesin SouthernAfricanadults.AIDS2008;22:2117-25.20.PalmonR,KooBC,ShoultzDA,DieterichDT.Lackofhepatotoxicityassociated withnonnucleosidereversetranscriptaseinhibitors.JAcquirImmuneDeficSyndr2002;29:340-5.21.PatelAK,PujariS,PatelK,Patel J,ShahN,PatelB,GupteN.NevirapineversusefavirenzbasedantiretroviraltreatmentinnaiveIndianpatients:comparisonof effectivenessinclinicalcohort.JAssocPhysiciansIndia2006;54:915-18.22.SanneI,Mommeja-MarinH,HinkleJ,BartlettJA, LedermanMM,MaartensG,WakefordC,ShawA,QuinnJ,GishRG,RousseauF.Severehepatotoxicityassociatedwithnevirapine useinHIV-infectedsubjects.JInfectDis2005;191:825-9.23.ShiptonLK,WesterCW,StockS,NdwapiN,GaolatheT,ThiorI,Avalos A,MoffatHJ,MboyaJJ,WidenfeltE,EssexM,HughesMD,ShapiroRL.Safetyandefficacyofnevirapine-andefavirenz-based antiretroviraltreatmentinadultstreatedforTB-HIVco-infectioninBotswana.IntJTubercLungDis2009;13:360-6.24.VarmaJ, NateniyomS,AkksilpS,MankatitthamW,SirinakC,SattayawuthipongW,BurapatC,KittikraisakW,MonkongdeeP,CainKP,WellsCD, TapperoJW.HIVcareandtreatmentfactorsassociatedwithsurvivalduringTBtreatmentinThailand:anobservationalstudy.BMC InfectDis2009;9:42.
- 106. 98 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach Authors: GeorgeRutherford,AlicenSpaulding Date: 8Oct2009 Question: ShouldTDFvsABCbeusedforinitialART?(randomizedclinicaltrials) Settings: Multiplelocations Bibliography: 1.SaxP,TierneyC,CollierA,FischlM,GodfreyC,JahedN,DrollK,PeeplesL,MyersL,ThalG,RooneyJ,HaB, WoodwardW,DaarE.ACTG5202:shortertimetovirologicfailure(VF)withabacavir/lamivudine(ABC/3TC)than tenofovir/emtricitabine(TDF/FTC)aspartofcombinationtherapyintreatment-naïvesubjectswithscreeningHIVRNA ≥100,000c/mL[AbstractTHAB0303].XVIIInternationalConferenceonAIDS,MexicoCity,August3-8,2008.2.Smith KY,PatelP,FineD,BellosN,SloanL,LackeyP,KumarPN,Sutherland-PhillipsDH,Vavro,C,YauL,WannamakerP, ShaeferMS,HEATStudyTeam.Randomized,double-blind,placebo-matched,multicentertrialofabacivr/lamivudine ortenofovir/emtricitabinewithlopinavir/ritonavirforinitialHIVtreatment.AIDS2009;Jul31;23(12):1547-56. Qualityassessment Summaryoffindings Importance No.ofpatientsEffect Quality No.of stud- ies DesignLimitations Inconsis- tency Indirect- ness Impreci- sion Other consider- ations TDFABC Relative (95%CI) Absolute Mortality–notreported 0-----None0/0(0%)0/0(0%)-- Clinicalresponse(follow-upmean96weeks) 1Random- izedtrials Noserious limitations Noserious inconsis- tency Serious1Serious2None3 1/345 (0.3%) 0/343(0%) RR2.98 (0.12to 72.96) 0moreper 1000(from 0fewerto0 more) ⊕⊕OO LOW CRITICAL Severeadverseevents(follow-upmean96weeks) 1Random- izedtrials Noserious limitations Noserious inconsis- tency Serious1Noserious imprecision None3 97/345 (28.1%) 103/343 (30%) RR0.94 (0.74to 1.18) 18fewer per1000 (from78 fewerto54 more) ⊕⊕⊕O MODER- ATE CRITICAL
- 108. 100 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach Authors: GeorgeRutherford,AlicenSpaulding Date: 8Oct2009 Question: ShouldTDFvs(d4TorAZT)beusedforinitialART?(randomizedclinicaltrials) Settings: Multiplelocations Bibliography: 1.GallantJE,StaszewskiS,PozniakAL,DeJesusE,SuleimanJM,MillerMD,CoakleyDF,LuB,TooleJJ,ChengAK; 903StudyGroup.EfficacyandsafetyoftenofovirDFvsstavudineincombinationtherapyinantiretroviral-naive patients:a3-yearrandomizedtrial.JAMA2004;292:191-201.2.GallantJE,DeJesusE,ArribasJR,PozniakAL, GazzardB,CampoRE,LuB,McCollD,ChuckS,EnejosaJ,TooleJJ,ChengAK;Study934Group.TenofovirDF, emtricitabine,andefavirenzvs.zidovudine,lamivudine,andefavirenzforHIV.NEnglJMed2006;354(3):251-60.3. ReyD,HoenB,ChavanetP,SchmittMP,HoizeyG,MeyerP,PeytavinG,SpireB,AllavenaC,DiemerM,MayT,Schmit JL,DuongM,CalvezV,LangJM.Highrateofearlyvirologicalfailurewiththeonce-dailytenofovir/lamivudine/ nevirapinecombinationinnaiveHIV-1-infectedpatients.JAntimicrobChemother2009;63:380-8 Qualityassessment Summaryoffindings Importance No.ofpatientsEffect Quality No. of stud- ies DesignLimitations Inconsis- tency Indirect- ness Impreci- sion Other consider- ations TDF (d4Tor ZDV) Relative (95%CI) Absolute Mortality(follow-upmean144weeks) 1Random- izedtrials Serious1,2Noserious inconsis- tency Noserious indirect- ness3 Serious4None 6/303(2%) 5/299 (1.7%) RR1.18 (0.37to 3.84) 3moreper 1000(from 11fewerto 47more) ⊕⊕OO LOW CRITICAL Clinicalresponse–notreported 0-----none0/0(0%)0/0(0%)-- Severeadverseevents(follow-up1studyat36weeks,1studyat48weeks,1studyat144weeks) 3Random- izedtrials Noserious limitations5 Noserious inconsis- tency Noserious indirect- ness3 Noserious imprecision None6 250/591 (42.3%) 247/595 (41.5%) OR1.04 (0.81to 1.34) 10more per1000 (from50 fewerto72 more) ⊕⊕⊕⊕ HIGH CRITICAL
- 110. 102 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach Authors: GeorgeRutherford,AlicenSpaulding Date: 8Oct2009 Question: ShouldTDFvs(d4TorAZT)beusedforinitialART?(observationalstudies) Settings: Multiplelocations Bibliography: 1.MocroftA,PhillipsAN,LedergerberB,KatlamaC,ChiesiA,GoebelFD,Knysz B,AntunesF,ReissP,LundgrenJD.Relationshipbetweenantiretroviralsused aspartofacARTregimenandCD4cellcountincreasesinpatientswith suppressedviremia.AIDS2006;20:1141-50. Qualityassessment Summaryoffindings Importance No.ofpatientsEffect Quality No.of stud- ies DesignLimitations Inconsis- tency Indirect- ness Impreci- sion Other consider- ations TDF (d4Tor AZT) Relative (95%CI) Absolute Immunologicalresponse(observational)(Betterindicatedbyhighervalues) 2Observa- tional studies Noserious limitations1 Noserious inconsis- tency Noserious indirect- ness Noserious impreci- sion2 None 361820377- MD6.33 lower(22.5 lowerto 9.84higher) ⊕⊕OO LOW IMPORTANT 1 Thisisfrom1studybutwith2comparisons. 2 NoneoftheincludedstudiesprovidedstandarddeviationsforthemeanoutcomesothesameestimatedSD valuewasusedforallstudies.
- 112. 104 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach Qualityassessment Summaryoffindings Importance No.ofpatientsEffect Quality No.of stud- ies DesignLimitations Inconsis- tency Indirect- ness Impreci- sion Other consider- ations ZDVd4T Relative (95%CI) Absolute Mortality(follow-up3studiesat48weeks,1studyat52weeks,1studyat96weeks1) 6Random- izedtrials Noserious limitations2 Noserious inconsis- tency Serious3Serious4Reporting bias53/593 (0.5%) 5/586 (0.9%) RR0.74 (0.18to 2.93) 2fewerper 1000(from 7fewerto 16more) ⊕OOO VERYLOW CRITICAL Clinicalresponse(follow-up3studiesat48weeks,2studiesat52weeks) 7Random- izedtrials Noserious limitations2 Noserious inconsis- tency Serious3Noserious imprecision Reporting bias58/360 (2.2%) 6/361 (1.7%) RR1.26 (0.46to 3.45) 4moreper 1000(from 9fewerto 41more) ⊕⊕OO LOW CRITICAL Severeadverseevents(follow-up4studiesat48weeks,3studiesat52weeks) 9Random- izedtrials Noserious limitations2 Noserious inconsis- tency Serious3Noserious imprecision Reporting bias5 137/680 (20.1%) 169/685 (24.7%) RR0.85 (0.71to 1.02) 37fewer per1000 (from72 fewerto5 more) ⊕⊕OO LOW CRITICAL Virologicalresponse(follow-up4studiesat48weeks,3studiesat52weeks,1studyat96weeks) 10Random- izedtrials Noserious limitations2 Noserious inconsis- tency Serious3Noserious imprecision Reporting bias5 396/771 (51.4%) 409/768 (53.3%) RR0.97 (0.89to 1.07) 16fewer per1000 (from59 fewerto37 more) ⊕⊕OO LOW CRITICAL Adherence/tolerability/retention(follow-up4studiesat48weeks,3studiesat52weeks,1studyat96weeks,1studyat144weeks) 12Random- izedtrials Noserious limitations2 Noserious inconsis- tency Serious3Noserious imprecision Reporting bias5 632/1081 (58.5%) 585/1078 (54.3%) RR1.08 (0.97to1.2) 43more per1000 (from16 fewerto 109more) ⊕⊕OO LOW CRITICAL
- 114. 106 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach Authors: GeorgeRutherford,AlicenSpaulding Date: 8Oct2009 Question: ShouldAZTvsd4TbeusedforinitialART?(observationalstudies) Settings: Multiplesettings Bibliography: 1.GeorgeC,YesodaA,JayakumarB,LalL.Aprospectivestudyevaluatingclinicaloutcomesandcostsofthree NNRTI-basedHAARTregimensinKerala,India.JClinPharmTher2009;34:33-40.2.LaurentC,BourgeoisA,Mpoudi- NgoléE,CiaffiL,KouanfackC,MougnutouR,NkouéN,CalmyA,Koulla-ShiroS,DelaporteE.Tolerabilityand effectivenessoffirst-lineregimenscombiningnevirapineandlamivudinepluszidovudineorstavudineinCameroon. AIDSResHumRetroviruses2008;24:393-9.3.MocroftA,PhillipsAN,LedergerberB,KatlamaC,ChiesiA,GoebelFD, KnyszB,AntunesF,ReissP,LundgrenJD.RelationshipbetweenantiretroviralsusedaspartofacARTregimenand CD4cellcountincreasesinpatientswithsuppressedviremia.AIDS2006;20:1141-50.4.NjorogeJ,ReidyW,John- StewartG,AttwaM,KiguruJ,NgumoR,WambuaN,ChungMH.Incidenceofperipheralneuropathyamongpatients receivingHAARTregimenscontainingstavudinevs.zidovudineinKenya[AbstractTUPEB179].5thConferenceonHIV PathogenesisandTreatmentandPrevention,CapeTown,SouthAfrica,19−22July2009.5.PazareAR,KhirsagarN, GogatayN,BajpaiS.Comparativestudyofincidenceofhyperlactetemia/lacticacidosisinstavudinevs.AZTbased regime[AbstractTHPE0159].XVIIInternationalAIDSConference,MexicoCity,Mexico,3−8August2008. Qualityassessment Summaryoffindings Importance No.ofpatientsEffect Quality No.of stud- ies DesignLimitations Inconsis- tency Indirect- ness Impreci- sion Other consider- ations AZTd4T Relative (95%CI) Absolute Mortality(observational) 1Observa- tional studies Noserious limitations Noserious inconsis- tency Noserious indirect- ness Noserious imprecision None 8/85(9.4%) 11/84 (13.1%) RR0.72 (0.3to1.7) 37fewer per1000 (from92 fewerto92 more) ⊕⊕OO LOW CRITICAL
- 116. 108 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach Monitoringstrategiesforguidingwhentoswitch Authors: LarryWilliamChang,JamalHarris Date: 12Aug2009 Question: Shouldclinicalmonitoringvsimmunologicalandclinicalmonitoringbeusedinguidingwhentoswitchfirst-line antiretroviraltherapyinadultsinlow-resourcesettings? Settings: Low-resourcesettings Bibliography: HBAC2008,DART2009 Qualityassessment Summaryoffindings Impor- tance No.ofpatientsEffect Quality No. of stud- ies DesignLimitations Inconsis- tency Indirect- ness Impreci- sion Other consider- ation Clinical monitoring Immuno- logicaland Clinical Monitoring Relative (95%CI) Absolute Mortality(follow-upmedian3-5years) 2Random- ized izedtrials Serious1Noserious inconsis- tency Noserious indirect- ness2 Serious3None4 ?/20375?/20275 HR1.35 (1.12to 1.63) - ⊕⊕OO LOW CRITICAL AIDS-definingillness–notreported 0----------CRITICAL AIDS-definingillnessormortality(follow-upmedian3-5years) 2Random- izedtrials Serious1Noserious inconsis- tency Noserious indirect- ness2 Noserious imprecision None4 547/2037 (26.9%)6 414/2027 (20.4%)6 HR1.33 (1.16to 1.51) 58more per1000 (from29 moreto88 more) ⊕⊕⊕O MODER- ATE CRITIC-AL Seriousadverseevent(follow-upmedian5years) 17Random- izedtrials Serious1Noserious inconsist- ency Noserious indirect- ness2 Serious3None4 ?/16608?/16568 HR1.12 (0.94to 1.31) - ⊕⊕OO LOW CRITICAL
- 118. 110 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach Authors: LarryWilliamChang,JamalHarris Date: 12Aug2009 Question: Shouldclinicalmonitoringvsvirological,immunological,andclinicalmonitoringbeusedforguidingwhentoswitch first-lineantiretroviraltherapyinadultsinlow-resourcesettings? Settings: Low-resourcesettings Bibliography: HBAC2008 Qualityassessment Summaryoffindings Importance NoofpatientsEffect Quality No. of stud- ies DesignLimitations Inconsis- tency Indirect- ness Imprecis- ion Other consider- ations Clinical monitoring Virologi- cal, immuno- logical, and clinical monitoring Relative (95%CI) Absolute Mortality(follow-upmedian3years) 1Random- izedtrials Serious1Noserious inconsis- tency Noserious indirect- ness2 Serious3None4 ?/3775?/3685HR1.58 (0.97to2.6) - ⊕⊕OO LOW CRITICAL AIDS-definingillness–notreported 0----------CRITICAL AIDS-definingillnessormortality(follow-upmedian3years) 1Random- izedtrials Serious1Noserious inconsis- tency Noserious indirect- ness2 Serious3None4 72/377 (19.1%)6 47/368 (12.8%)6 HR1.88 (1.25to 2.84) 99more per1000 (from29 moreto194 more) ⊕⊕OO LOW CRITICAL Unnecessaryswitch(switchtosecond-linetherapywithundetectableviralload)(follow-upmedian3years) 1Random- izedtrials Serious1Noserious inconsis- tency Noserious indirect- ness2 Serious3None4 15/377(4%)0/368(0%) RR30.3 (1.82to 504) - ⊕⊕OO LOW CRITICAL
- 120. 112 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach Authors: LarryWilliamChang,JamalHarris Date: 12Aug2009 Question: Shouldclinicalandimmunologicalmonitoringvsvirological,immunologicalandclinicalmonitoringbeusedinguiding whentoswitchfirst-lineantiretroviraltherapyinadultsinlow-resourcesettings? Settings: Low-resourcesettings. Bibliography: H.B.A.C.2008 Qualityassessment Summaryoffindings Importance No.ofpatientsEffect Quality No. of stud- ies DesignLimitations Inconsis- tency Indirect- ness Impreci- sion Other consider- ations Clinical and immuno- logical monitoring Virologi- cal, immuno- logicaland clinical monitoring Relative (95%CI) Absolute Mortality(follow-upmedian3years) 1Random- izedtrials Serious1Noserious inconsis- tency Noserious indirect- ness2 Serious3None4 ?/3715?/3685HR1.14(0.7 to1.9) - ⊕⊕OO LOW CRITICAL AIDS-definingillness–notreported 0----------CRITICAL AIDS-definingillnessormortality(follow-upmedian3years) 1Random- izedtrials Serious1Noserious inconsis- tency Noserious indirect- ness2 Serious3None4 58/371 (15.6%)6 47/368 (12.8%) HR1.28 (0.84to 1.97) 33more per1000 (from19 fewerto 108more) ⊕⊕OO LOW CRITICAL Unncessaryswitch(switchtosecond-linetherapywithundetectableviralload)(follow-upmedian3years) 1Random- izedtrials Serious1Noserious inconsis- tency Noserious indirect- ness2 Very serious7 None4 0/371(0%)0/368(0%) Not estim-able - ⊕OOO VERYLOW CRITICAL
- 122. 114 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach Authors: LarryWilliamChang,JamalHarris Date: 14Sep2009 Question: Shouldvirological,immunological,andclinicalmonitoringvsimmunologicalandclinicalmonitoringbeusedin guidingwhentoswitchfirst-lineantiretroviraltherapyinadultsinlow-resourcesettings? Settings: Low-resourcesettings. Bibliography: ARTLINC2006,2008 Qualityassessment Summaryoffindings Impor- tance NoofpatientsEffect Quality No. of stud- ies DesignLimitations Inconsis- tency Indirect- ness Impreci- sion Other consider- ations Virologi- cal, immuno- logicaland clinical monitoring Immuno- logicaland clinical monitoring Relative (95%CI) Absolute Mortality(follow-up12months) 1Observ- ational studies Serious1Noserious inconsis- tency Noserious indirect- ness Noserious imprecision None See comment2 See comment2 HR2.28 (0.76to 6.79) - ⊕OOO VERYLOW CRITICAL Rateofswitching 1Observ- ational studies Serious3Noserious inconsis- tency Noserious indirect- ness Noserious imprecision None 236/6369 (3.7%) 340/13744 (2.5%) RR1.60 (1.35to 1.89)4 15moreper 1000(from 9moreto 22more) ⊕OOO VERYLOW Timetoswitch(7-18months) 1Observ- ational studies Serious3Noserious inconsis- tency Noserious indirect- ness Noserious imprecision None ?/63695?/137445 HR1.38 (0.97to 1.98) - ⊕OOO VERYLOW Timetoswitch(19-30months) 1Observ- ational studies Serious3Noserious inconsis- tency Noserious indirect- ness Noserious imprecision None ?/27015?/64885HR0.97 (0.58to1.6) - ⊕OOO VERYLOW
- 124. 116 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach Whattouseinsecond-line Authors: HumphreysEandHarrisJ Date: 21Aug2009 Question: Shouldlamivudine(3TC)bemaintainedinsecond-lineantiretroviralregimensforpatientsfailingfirst-linetherapy? Bibliography: FoxZ,DragstedU,GerstoftJ,etal.Arandomizedtrialtoevaluatecontinuationversusdiscontinuationoflamivudine inindividualsfailingalamivudine-containingregimen:theCOLATEtrial.Antiviraltherapy2006;11(6):761-770. Qualityassessment Summaryoffindings Importance No.ofpatientsEffect Quality No. of stud- ies DesignLimitations Inconsis- tency Indirect- ness Impreci- sion Other consider- ations Maintain- ing3TCin 2ndline No3TCin 2ndline (control) Relative (95%CI) Absolute Mortality–notmeasured1 0-------CRITICAL Progressionofdisease–notmeasured 0-------CRITICAL Severeadverseevents(follow-up48weeks) 1Random- izedtrials Noserious limitations3 Noserious inconsis- tency Serious4Serious5None -- Not estimable2 ⊕⊕OO LOW CRITICAL Adherence/tolerability/retention–notreported 0-------CRITICAL Virologicalresponse(follow-up48weeks;measuredas:meanreductionfrombaselinelog10copies/mlofHIVRNA;betterindicatedbyhighervalues) 1Random- izedtrials Noserious limitations Noserious inconsis- tency Serious4Serious5None 28627- MD0.4 lower(0.87 lowerto 0.07higher) ⊕⊕OO LOW IMPORTANT
- 126. 118 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach Question: ShouldPImonotherapybeusedforpatientsfailingfirst-linetherapy? Bibliography: Arribas2005;Arribas2009a;Arribas2009b;Cameron2008;Delfraissy2008;Guttmann2008;Katlama2009;Nunes 2007;Singh2007;Waters2008. Qualityassessment Summaryoffindings Importance No.ofpatientsEffect Quality No. of stud- ies DesignLimitations Inconsis- tency Indirect- ness Impreci- sion Other consider- ations PI monother- apy cART Relative (95%CI) Absolute Mortality(follow-up96weeks) 2Random- izedtrials Noserious limitations1 Noserious inconsis- tency Serious2Serious3None4 3/207 (1.4%) 1/153 (0.7%) RR1.46 (0.22to 9.8) 3moreper 1000(from 5fewerto 58more) ⊕⊕OO LOW CRITICAL Clinicaldiseaseprogression–notreported 0-----none----CRITICAL Seriousadverseevents(grade3or4adverseevent;follow-up1study24weeks,4studies48weeks,2studies96weeks)5 7Random- izedtrials Serious1Noserious inconsis- tency Serious2Serious3None 25/499(5%) 26/472 (5.5%) RR1.02 (0.5to2.07) 1moreper 1000(from 28fewerto 59more) ⊕OOO VERYLOW CRITICAL Adherence/tolerability/retention(proportiononrandomizedtreatmentatstudyend;follow-up1study24weeks,4studiesat48weeks,3studiesat96weeks) 8Random- izedtrials Noserious limitations1 Noserious inconsis- tency Serious2Noserious imprecision None 506/607 (83.4%) 448/529 (84.7%) RR0.99 (0.95to 1.04) 8fewerper 1000(from 42fewerto 34more) ⊕⊕⊕O MODER- ATE CRITICAL Virologicalresponse(proportionwithHIVRNA<50copies/mlorlowestreportedvalue;follow-up6studies48weeks,3studies96weeks) 9Random- izedtrials Noserious limitations1 Noserious inconsis- tency Serious2Noserious imprecision None 470/636 (73.9%) 460/560 (82.1%) RR0.94 (0.89to 0.99) 49fewer per1000 (from8 fewerto90 fewer) ⊕⊕⊕O MODER- ATE IMPORTANT
- 128. 120 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach Question: Shouldatazanavir/ritonavirvs.lopinavir/ritonavirbeusedforpatientsfailingfirst-linetherapy? Bibliography: MolinaJM,Andrade-VillanuevaJ,EchevarriaJ,etal.Once-dailyatazanavir/ritonavirversustwice-dailylopinavir/ ritonavir,eachincombinationwithtenofovirandemtricitabine,formanagementofantiretroviral-naiveHIV-1-infected patients:48weekefficacyandsafetyresultsoftheCASTLEstudy.Lancet2008;372:646-55.MolinaJM,Andrade- VillanuevaJ,EchevarriaJ,etal.Atazanavir/ritonavirvs.lopinavir/ritonavirinantiretroviralnaiveHIV-1-infectedpatients: CASTLE96-weekefficacyandsafety.48tthAnnualICAAC/IDSAMeeting,October25−28,2008,WashingtonDC. AbstractH-1250d. Qualityassessment Summaryoffindings Importance No.ofpatientsEffect Quality No. of stud- ies DesignLimitations Inconsis- tency Indirect- ness Impreci- sion Other consider- ations Atazanavir/ ritonavir Lopinavir/ ritonavir Relative (95%CI) Absolute Mortality(follow-up48weeks) 1Random- izedtrials Noserious limitations1 Noserious inconsis- tency Serious indirect- ness2 Serious3None 6/440 (1.4%) 6/443 (1.4%) RR1.01 (0.33to3.1) 0moreper 1000(from 9fewerto 28more) ⊕⊕OO LOW CRITICAL Severeadverseevents(follow-up96weeks)4 1Random- izedtrials Serious1Noserious inconsis- tency Serious indirect- ness2 Serious3None 63/441 (14.3%) 50/437 (11.4%) RR1.25 (0.88to 1.77) 29more per1000 (from14 fewerto88 more) ⊕OOO VERYLOW CRITICAL Clinicaldiseaseprogression–notreported 0-------CRITICAL Adherence/tolerability/retention(follow-up48weeks;adherencequestionnaire) 1Random- izedtrials Serious1Noserious inconsis- tency Serious indirect- ness2 Noserious imprecision None 330/440 (75%) 316/443 (71.3%) RR1.05 (0.97to 1.14) 36more per1000 (from21 fewerto 100more) ⊕⊕OO LOW CRITICAL
- 130. 122 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach Question: Shoulddarunavir/ritonavirvs.lopinavir/ritonavirbeusedforpatientsfailingfirst-linetherapy? Settings: Bibliography: MillsAM,NelsonM,JayaweeraD,etal.Once-dailydarunavir/ritonavirvs.lopinavir/ritonavirintreatment-naive,HIV-1- infectedpatients:96weekanalysis.AIDS2009;23:1679-88. Qualityassessment Summaryoffindings Importance No.ofpatientsEffect Quality No. of stud- ies DesignLimitations Inconsis- tency Indirect- ness Impreci- sion Other consider- ations Darunavir/ ritonavir Lopinavir/ ritonavir Relative (95%CI) Absolute Mortality(follow-up96weeks) 1Random- izedtrials Noserious limitations1 Noserious inconsis- tency Serious indirect- ness3 Serious2None 1/343 (0.3%) 5/346 (1.4%) RR0.2 (0.02to 1.72) 12fewer per1000 (from14 fewerto10 more) ⊕⊕OO LOW CRITICAL Severeadverseevents(follow-up96weeks)4 1Random- izedtrials Serious1Noserious inconsis- tency Serious indirect- ness3 Noserious imprecision None 34/343 (9.9%) 55/346 (15.9%) RR0.62 (0.42to 0.93) 60fewer per1000 (from11 fewerto92 fewer) ⊕⊕OO LOW CRITICAL Clinicaldiseaseprogression–notreported 0-------CRITICAL Adherence/tolerability/retention(follow-up96weeks;reportedasretention,numberstillonrandomizedstudydrug5) 1Random- izedtrials Noserious limitations1 Noserious inconsis- tency Serious indirect- ness3 Noserious imprecision None 284/343 (82.8%) 265/346 (76.6%) RR1.08(1 to1.17) 61more per1000 (from0 moreto130 more) ⊕⊕⊕O MODER- ATE IMPORTANT
- 132. 124 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach Question: Shouldfos-amprenavir/ritonavirvs.lopinavir/ritonavirbeusedforpatientsfailingfirst-linetherapy? Settings: Bibliography: EronJ,YeniP,GatheJetal.TheKLEANstudyoffosamprenavir-ritonavirversuslopinavir-ritonavir,eachincombination withabacavir-lamivudine,forinitialtreatmentofHIVinfectionover48weeks:arandomisednon-inferioritytrial.Lancet 2006;368:476-82. Qualityassessment Summaryoffindings Importance No.ofpatientsEffect Quality No. of stud- ies DesignLimitations Inconsis- tency Indirect- ness Impreci- sion Other consider- ations Fosampre- navir/ ritonavir Lopinavir/ ritonavir Relative (95%CI) Absolute Mortality(follow-upmedian48weeks) 1Random- izedtrials Noserious limitations1 Noserious inconsis- tency Serious2Serious3None 4/443 (0.9%) 1/444 (0.2%) RR4.01 (0.45to 35.73) 7moreper 1000(from 1fewerto 78more) ⊕⊕OO LOW CRITICAL Severeadverseevents(follow-upmedian48weeks;adverseeventsleadingtodiscontinuation) 1Random- izedtrials Serious1Noserious inconsis- tency Serious2Serious3None 53/436 (12.2%) 43/443 (9.7%) RR1.25 (0.86to 1.83) 24more per1000 (from14 fewerto81 more) ⊕OOO VERYLOW CRITICAL Clinicaldiseaseprogressionordeath(follow-upmedian48weeks) 1Random- izedtrials Noserious limitations1 Noserious inconsis- tency Serious2Serious3None 11/443 (2.5%) 11/444 (2.5%) RR1(0.44 to2.29) 0fewerper 1000(from 14fewerto 32more) ⊕⊕OO LOW CRITICAL Adherence/tolerability/retention(follow-upmedian48weeks;adherencebypillcountsreportedasmedianpercentage) 1Random- izedtrials Serious1Noserious inconsis- tency Serious2Noserious imprecision None 427/443 (96.4%) 435/444 (98%) RR0.98 (0.96to 1.01) 20fewer per1000 (from39 fewerto10 more) ⊕⊕OO LOW CRITICAL
- 134. 126 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach 1. WHO. Antiretroviral treatment working group treatment white paper. 2010. 2. Siegfried NL, Uthman OA, Rutherford GW. Optimal time for initiation of antiretroviral therapy for asymptomatic, HIV-infected, treatment-naive adults. Cochrane Database of Systematic Reviews 2010. 2010(Issue 2 (In press)). 3. Severe P, Pape J, Fitzgerald D, et al. A randomized clinical trial of early versus standard antiretroviral therapy for HIV-infected patients with a CD4 cell count of 200-350 cells/mm3 (CIPRATH-001). 49th Interscience Conference on Antimicrobial Agents and Chemotherpy, San Fransisco, 2009. 4. Emery S, Neuhaus JA, Phillips AN, Babiker A, Cohen CJ, Gatell JM, et al. Major clinical outcomes in antiretroviral therapy (ART)-naive participants and in those not receiving ART at baseline in the SMART study. J Infect Dis 2008;197(8):1133-44. 5. Sterne JA, May M, Costagliola D, de Wolf F, Phillips AN, Harris R, et al. Timing of initiation of antiretroviral therapy in AIDS-free HIV-1-infected patients: a collaborative analysis of 18 HIV cohort studies. Lancet 2009;373(9672):1352-63. 6. Moh R, Danel C, Messou E, Ouassa T, Gabillard D, Anzian A, et al. Incidence and determinants of mortality and morbidity following early antiretroviral therapy initiation in HIV-infected adults in West Africa. AIDS 2007;21(18):2483-91. 7. Badri M, Bekker LG, Orrell C, Pitt J, Cilliers F, Wood R. Initiating highly active antiretroviral therapy in sub-Saharan Africa: an assessment of the revised World Health Organization scaling-up guidelines. AIDS 2004;18(8):1159-68. 8. Wong KH, Chan KC, Cheng KL, Chan WK, Kam KM, Lee SS. Establishing CD4 thresholds for highly active antiretroviral therapy initiation in a cohort of HIV-infected adult Chinese in Hong Kong. AIDS Patient Care STDS 2007;21(2):106-15. 9. UNAIDS. Cost estimates: AIDS financing and economics. 2009. 10. Granich RM, Gilks CF, Dye C, De Cock KM, Williams BG. Universal voluntary HIV testing with immediate antiretroviral therapy as a strategy for elimination of HIV transmission: a mathematical model. Lancet 2009 Jan 3;373(9657):48-57. 11. Danel C, Moh R, Minga A, Anzian A, Ba-Gomis O, Kanga C, et al. CD4-guided structured antiretroviral treatment interruption strategy in HIV-infected adults in west Africa (Trivacan ANRS 1269 trial): a randomised trial. Lancet 2006;367(9527):1981-9. 12. Havlir DV, Getahun H, Sanne I, Nunn P. Opportunities and challenges for HIV care in overlapping HIV and TB epidemics. JAMA 2008;300(4):423-30. 13. Lawn SD, Churchyard G. Epidemiology of HIV-associated tuberculosis. Curr Opin HIV AIDS 2009;4(4):325-33. 14. Hammer SM, Eron JJ, Jr., Reiss P, Schooley RT, Thompson MA, Walmsley S, et al. Antiretroviral treatment of adult HIV infection: 2008 recommendations of the International AIDS Society-USA panel. JAMA 2008;300(5):555-70. 22. References
- 135. 127 15. Gange SJ, Kitahata MM, Saag MS, Bangsberg DR, Bosch RJ, Brooks JT, et al. Cohort profile: the North American AIDS Cohort Collaboration on Research and Design (NA- ACCORD). Int J Epidemiol 2007;36(2):294-301. 16. Ngoma D, Makombe SD, Kamoto K, Harries AD. World Health Organization Clinical Stage 3 disease conditions in HIV-infected patients who start antiretroviral therapy in Malawi. Trop Doct 2008;38(3):159-60. 17. Teck R, Ascurra O, Gomani P, Manzi M, Pasulani O, Kusamale J, et al. WHO clinical staging of HIV infection and disease, tuberculosis and eligibility for antiretroviral treatment: relationship to CD4 lymphocyte counts. Int J Tuberc Lung Dis 2005;9(3):258-62. 18. Edathodu J, Ali B, Alrajhi AA. CD4 validation for the World Health Organization classification and clinical staging of HIV/AIDS in a developing country. Int J Infect Dis 2009;13(2):243-6. 19. Kassa E, Rinke de Wit TF, Hailu E, Girma M, Messele T, Mariam HG, et al. Evaluation of the World Health Organization staging system for HIV infection and disease in Ethiopia: association between clinical stages and laboratory markers. AIDS 1999;13(3):381-9. 20. Annam V, Yelikar BR, Inamadar AC, Palit A. Histopathological study of pruritic papular eruptions in HIV-infected patients in relationship with CD4, CD8 counts. Indian J Pathol Microbiol 2009;52(3):321-4. 21. Lakshmi SJ, Rao GR, Rao KA, Prasad PG, Kumar YH. Pruritic papular eruptions of HIV: a clinicopathologic and therapeutic study. Indian J Dermatol Venereol Leprol 2008;74(5):501- 3. 22. WHO. Guidance on provider-initiated HIV testing and counselling in health facilities. 2007. 23. Hoffmann CJ, Charalambous S, Sim J, Ledwaba J, Schwikkard G, Chaisson RE, et al. Viremia, resuppression, and time to resistance in human immunodeficiency virus (HIV) subtype C during first-line antiretroviral therapy in South Africa. Clin Infect Dis 2009;49(12):1928-35. 24. Amin J, Moore A, Carr A, French MA, Law M, Emery S, et al. Combined analysis of two- year follow-up from two open-label randomized trials comparing efficacy of three nucleoside reverse transcriptase inhibitor backbones for previously untreated HIV-1 infection: OzCombo 1 and 2. HIV clinical trials 2003;4(4):252-61. 25. French M, Amin J, Roth N, Carr A, Law M, Emery S, et al. Randomized, open-label, comparative trial to evaluate the efficacy and safety of three antiretroviral drug combinations including two nucleoside analogues and nevirapine for previously untreated HIV-1 Infection: the OzCombo 2 study. HIV clinical trials 2002;3(3):177-85. 26. Eron JJ, Jr., Murphy RL, Peterson D, Pottage J, Parenti DM, Jemsek J, et al. A comparison of stavudine, didanosine and indinavir with zidovudine, lamivudine and indinavir for the initial treatment of HIV-1 infected individuals: selection of thymidine analog regimen therapy (START II). AIDS 2000;14(11):1601-10.
- 136. 128 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach 27. Gathe J, Jr., Badaro R, Grimwood A, Abrams L, Klesczewski K, Cross A, et al. Antiviral activity of enteric-coated didanosine, stavudine, and nelfinavir versus zidovudine plus lamivudine and nelfinavir. J Acquir Immune Defic Syndr 2002;31(4):399-403. 28. Carr A, Chuah J, Hudson J, French M, Hoy J, Law M, et al. A randomised, open-label comparison of three highly active antiretroviral therapy regimens including two nucleoside analogues and indinavir for previously untreated HIV-1 infection: the OzCombo1 study. AIDS 2000;14(9):1171-80. 29. Geijo Martínez MP MMM, Solera Santos J, Barberá Farré JR, Rodríguez Zapata M, Marcos Sánchez F, Martínez Alfaro E, Cuadra García-Tenorio F, Sanz Moreno J, Moreno Mendaña JM, Beato Pérez JL, Sanz Sanz J; GECMEI. Ensayo clínico comparativo de eficacia y seguridad de cuatro pautas de tratamiento antirretroviral de alta eficacia (TARGA) en pacientes con infección por VIH avanzada [Test comparative clinical efficacy and safety of four treatment guidelines highly active antiretroviral (TARGA) in patients with advanced HIV infection]. Rev Clin Esp 2006;206:67-76. 30. Kumar PN, Rodriguez-French A, Thompson MA, Tashima KT, Averitt D, Wannamaker PG, et al. A prospective, 96-week study of the impact of Trizivir, Combivir/nelfinavir, and lamivudine/stavudine/nelfinavir on lipids, metabolic parameters and efficacy in antiretroviral-naive patients: effect of sex and ethnicity. HIV Med 2006;7(2):85-98. 31. Li T, Dai Y, Kuang J, Jiang J, Han Y, Qiu Z, et al. Three generic nevirapine-based antiretroviral treatments in Chinese HIV/AIDS patients: multicentric observation cohort. PLoS ONE 2008;3(12):e3918. 32. Robbins GK, De Gruttola V, Shafer RW, Smeaton LM, Snyder SW, Pettinelli C, et al. Comparison of sequential three-drug regimens as initial therapy for HIV-1 infection. N Engl J Med 2003;349(24):2293-303. 33. Squires KE, Gulick R, Tebas P, Santana J, Mulanovich V, Clark R, et al. A comparison of stavudine plus lamivudine versus zidovudine plus lamivudine in combination with indinavir in antiretroviral naive individuals with HIV infection: selection of thymidine analog regimen therapy (START I). AIDS 2000;14(11):1591-600. 34. The Adult Antiretroviral Treatment and Resistance Study Tshepo [database on the Internet] 2009 [cited November 11, 2009]. Available from: http://clinicaltrials.gov/ct2/show/ NCT00197613?term=Tshepo&rank=1. 35. Gallant JE, Staszewski S, Pozniak AL, DeJesus E, Suleiman JM, Miller MD, et al. Efficacy and safety of tenofovir DF vs stavudine in combination therapy in antiretroviral-naive patients: a 3-year randomized trial. JAMA 2004;292(2):191-201. 36. Rey D, Hoen B, Chavanet P, Schmitt MP, Hoizey G, Meyer P, et al. High rate of early virological failure with the once-daily tenofovir/lamivudine/nevirapine combination in naive HIV-1-infected patients. J Antimicrob Chemother 2009;63(2):380-8.
- 137. 129 37. Arribas JR, Pozniak AL, Gallant JE, Dejesus E, Gazzard B, Campo RE, et al. Tenofovir disoproxil fumarate, emtricitabine, and efavirenz compared with zidovudine/lamivudine and efavirenz in treatment-naive patients: 144-week analysis. J Acquir Immune Defic Syndr 2008;47(1):74-8. 38. Lapadula G, Costarelli S, Quiros-Roldan E, Calabresi A, Izzo I, Carosi G, et al. Risk of early virological failure of once-daily tenofovir-emtricitabine plus twice-daily nevirapine in antiretroviral therapy-naive HIV-infected patients. Clin Infect Dis 2008;46(7):1127-9. 39. Towner W, Kerrigan HL, LaRivière M, et al. eds. Efficacy of a once-daily regimen of nevirapine(NVP), lamivudine (3TC) and tenofovir (TDF) in treatment-naive HIV-infected patients: a pilot study. Seventh International Congress on Drug Therapy in HIV Infection; 2004. 40. Vicente Soriano SK, Horacio Migrone et al, editors. Prospective randomised comparison of nevirapine and atazanavir/ritonavir both combined with tenofovir DF/emtricitabine in treatment-naive HIV-1 infected patients: ARTEN Study, week 48 results. 5th IAS Conference on HIV Pathogenesis, Treatment and Prevention; 19-22 July 2009; Cape Town, South Africa. 41. Alexandra Calmy AN, J Lange, M Battegay, F de Wolf, P Reiss, B Hirschel, F Wit, and for the Swiss HIV Cohort Study and the Netherlands ATHENA Observational Cohort, eds. Nevirapine administered once daily is as efficient as a twice-daily dosing. A collaborative cohort study. 15th Conference on Retroviruses and Opportunistic Infecions; 2009; Boston. 42. Havlir DV, Koelsch KK, Strain MC, Margot N, Lu B, Ignacio CC, et al. Predictors of residual viremia in HIV-infected patients successfully treated with efavirenz and lamivudine plus either tenofovir or stavudine. J Infect Dis 2005;191(7):1164-8. 43. Lodwick RK, Smith CJ, Youle M, Lampe FC, Tyrer M, Bhagani S, et al. Stability of antiretroviral regimens in patients with viral suppression. AIDS 2008;22(9):1039-46. 44. Willig JH, Abroms S, Westfall AO, Routman J, Adusumilli S, Varshney M, et al. Increased regimen durability in the era of once-daily fixed-dose combination antiretroviral therapy. AIDS 2008;22(15):1951-60. 45. Mocroft A, Phillips AN, Ledergerber B, Katlama C, Chiesi A, Goebel FD, et al. Relationship between antiretrovirals used as part of a cART regimen and CD4 cell count increases in patients with suppressed viremia. AIDS 2006;20(8):1141-50. 46. Wolbers M, Battegay M, Hirschel B, Furrer H, Cavassini M, Hasse B, et al. CD4+ T-cell count increase in HIV-1-infected patients with suppressed viral load within 1 year after start of antiretroviral therapy. Antivir Ther 2007;12(6):889-97. 47. Sanchez-de la Rosa R, Herrera L, Moreno S. Cost-effectiveness analysis of emtricitabine/ tenofovir versus lamivudine/zidovudine, in combination with efavirenz, in antiretroviral- naive, HIV-1-infected patients. Clin Ther 2008;30(2):372-81.
- 138. 130 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach 48. Fernandez Lison LC. PDLLE, Hevia Alonso A, Garrido Martinez MT, Bocanegra Martin C. Cost-effectiveness analysis of tenofovir versus zidovudine in combination therapy with efavirenz and lamivudine for the treatment of HIV in naive patients. Farmacia Hospitalaria 2005(29):11-7. 49. Ayala Gaytan JJ dlGE, Garcia MC, Chavez SBV. Nevirapine or efavirenz in combination with two nucleoside analogues in HIV infected antiretroviral naïve patients. Med Intern Mex 2004;20:24. 50. Manosuthi W, Sungkanuparph S, Tantanathip P, Lueangniyomkul A, Mankatitham W, Prasithsirskul W, et al. A randomized trial comparing plasma drug concentrations and efficacies between 2 nonnucleoside reverse-transcriptase inhibitor-based regimens in HIV-infected patients receiving rifampicin: the N2R Study. Clin Infect Dis 2009;48(12):1752- 9. 51. Nuñez M, Soriano V, Martin-Carbonero L, Barrios A, Barreiro P, Blanco F, et al. SENC (Spanish efavirenz vs. nevirapine comparison) trial: a randomized, open-label study in HIV-infected naive individuals. HIV clinical trials 2002;3(3):186-94. 52. Sow PG BM, Diallo PD, Lo I, Ndiaye B, Gaye AM, editor. Efficacy and safety of lamivudine+zidovudine+efavirenz and lamivudine+zidovudine+névirapine in treatment HIV1 infected patients. A retrospective cross study analysis. XVI International AIDS Conference; 13-18 August 2006: Toronto, Canada. 53. van den Berg-Wolf M, Hullsiek KH, Peng G, Kozal MJ, Novak RM, Chen L, et al. Virologic, immunologic, clinical, safety, and resistance outcomes from a long-term comparison of efavirenz-based versus nevirapine-based antiretroviral regimens as initial therapy in HIV- 1-infected persons. HIV clinical trials 2008;9(5):324-36. 54. van Leth F, Phanuphak P, Ruxrungtham K, Baraldi E, Miller S, Gazzard B, et al. Comparison of first-line antiretroviral therapy with regimens including nevirapine, efavirenz, or both drugs, plus stavudine and lamivudine: a randomised open-label trial, the 2NN Study. Lancet 2004;363(9417):1253-63. 55. Clinicaltrials.gov. Comparison of nevirapine and efavirenz for the treatment of HIV-TB coInfected patients (ANRS 12146 CARINEMO). 2009; Available from: http://clinicaltrials. gov/ct2/show/NCT00495326?term=ANRS+12146&rank=1. 56. Evaluation of 4 new simplified antiretroviral treatments in naive HIV-1 infected patients in Africa (ANRS 12115 DAYANA) [database on the Internet] 2009. Available from: http:// clinicaltrials.gov/ct2/show/NCT00573001?term=DAYANA&rank=1. 57. Rajesh L, Karunaianantham R, Narayanan PR, Swaminathan S. Antiretroviral drug-resistant mutations at baseline and at time of failure of antiretroviral therapy in HIV type 1-coinfected TB patients. AIDS Res Hum Retroviruses 2009;25(11):1179-85. 58. Gilead Sciences. Viread prescribing information. 2010 (Revised 03/2010 ).
- 139. 131 59. Ananworanich J, Moor Z, Siangphoe U, Chan J, Cardiello P, Duncombe C, et al. Incidence and risk factors for rash in Thai patients randomized to regimens with nevirapine, efavirenz or both drugs. AIDS 2005;19(2):185-92. 60. Winston A, Pozniak A, Smith N, Fletcher C, Mandalia S, Parmar D, et al. Dose escalation or immediate full dose when switching from efavirenz to nevirapine-based highly active antiretroviral therapy in HIV-1-infected individuals? AIDS 2004;18(3):572-4. 61. Laureillard D, Prak N, Fernandez M, Ngeth C, Moeung S, Riel V, et al. Efavirenz replacement by immediate full-dose nevirapine is safe in HIV-1-infected patients in Cambodia. HIV Med 2008;9(7):514-8. 62. Isaakidis P, Raguenaud ME, Phe T, Khim SA, Kuoch S, Khem S, et al. Evaluation of a systematic substitution of zidovudine for stavudine-based HAART in a program setting in rural Cambodia. J Acquir Immune Defic Syndr 2008;49(1):48-54. 63. Ssali F, Stohr W, Munderi P, Reid A, Walker AS, Gibb DM, et al. Prevalence, incidence and predictors of severe anaemia with zidovudine-containing regimens in African adults with HIV infection within the DART trial. Antivir Ther 2006;11(6):741-9. 64. Amoroso A. Antiretroviral-associated drug toxicities leading to a switch in medication: Experience in Uganda, Kenya, and Zambia. 14th Conference on Retroviruses and Opportunistic Infections (CROI); 25-28 February 2007; Los Angeles, USA. 65. Fatu F, editor. Hematologic changes associated with zidovudine after single-drug substitution from stavudine in a home-based AIDS care program in rural Uganda. 15th 15th Conference on Retroviruses and Opportunistic Infections; 3-6 February 2008; Boston, USA. 66. Bannister WP, Ruiz L, Cozzi-Lepri A, Mocroft A, Kirk O, Staszewski S, et al. Comparison of genotypic resistance profiles and virological response between patients starting nevirapine and efavirenz in EuroSIDA. AIDS 2008;22(3):367-76. 67. Hitti J, Frenkel LM, Stek AM, Nachman SA, Baker D, Gonzalez-Garcia A, et al. Maternal toxicity with continuous nevirapine in pregnancy: results from PACTG 1022. J Acquir Immune Defic Syndr 2004;36(3):772-6. 68. Jamisse L, Balkus J, Hitti J, Gloyd S, Manuel R, Osman N, et al. Antiretroviral-associated toxicity among HIV-1-seropositive pregnant women in Mozambique receiving nevirapine- based regimens. J Acquir Immune Defic Syndr 2007;44(4):371-6. 69. Mocroft A, Staszewski S, Weber R, Gatell J, Rockstroh J, Gasiorowski J, et al. Risk of discontinuation of nevirapine due to toxicities in antiretroviral-naive and -experienced HIV- infected patients with high and low CD4+ T-cell counts. Antivir Ther 2007;12(3):325-33. 70. Lyons F, Hopkins S, Kelleher B, McGeary A, Sheehan G, Geoghegan J, et al. Maternal hepatotoxicity with nevirapine as part of combination antiretroviral therapy in pregnancy. HIV Med 2006;7(4):255-60.
- 140. 132 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach 71. Kiertiburanakul S, Sungkanuparph S, Charoenyingwattana A, Mahasirimongkol S, Sura T, Chantratita W. Risk factors for nevirapine-associated rash among HIV-infected patients with low CD4 cell counts in resource-limited settings. Curr HIV Res 2008;6(1):65-9. 72. Taiwo BO. Nevirapine toxicity. Int J STD AIDS 2006;17(6):364-9. 73. Knobel H, Guelar A, Montero M, Carmona A, Luque S, Berenguer N, et al. Risk of side effects associated with the use of nevirapine in treatment-naive patients, with respect to gender and CD4 cell count. HIV Med 2008;9(1):14-8. 74. Kondo W, Carraro EA, Prandel E, Dias JM, Perini J, Macedo RL, et al. Nevirapine-induced side effects in pregnant women: experience of a Brazilian university hospital. Braz J Infect Dis 2007;11(6):544-8. 75. Bonjoch A, Paredes R, Domingo P, Cervantes M, Pedrol E, Ribera E, et al. Long-term safety and efficacy of nevirapine-based approaches in HIV type 1-infected patients. AIDS Res Hum Retroviruses 2006;22(4):321-9. 76. De Lazzari E, Leon A, Arnaiz JA, Martinez E, Knobel H, Negredo E, et al. Hepatotoxicity of nevirapine in virologically suppressed patients according to gender and CD4 cell counts. HIV Med 2008;9(4):221-6. 77. Torti C, Costarelli S, De Silvestri A, Quiros-Roldan E, Lapadula G, Cologni G, et al. Analysis of severe hepatic events associated with nevirapine-containing regimens: CD4+ T-cell count and gender in hepatitis C seropositive and seronegative patients. Drug Saf 2007;30(12):1161-9. 78. Manfredi R, Calza L. Nevirapine versus efavirenz in 742 patients: no link of liver toxicity with female sex, and a baseline CD4 cell count greater than 250 cells/microl. AIDS 2006;20(17):2233-6. 79. Manfredi R, Calza L. Safety issues about nevirapine administration in HIV-infected pregnant women. J Acquir Immune Defic Syndr 2007;45(3):365-8. 80. Phanuphak N, Apornpong T, Teeratakulpisarn S, Chaithongwongwatthana S, Taweepolcharoen C, Mangclaviraj S, et al. Nevirapine-associated toxicity in HIV-infected Thai men and women, including pregnant women. HIV Med 2007;8(6):357-66. 81. Kumarasamy N, Venkatesh KK, Devaleenal B, Palanivel V, Cecelia AJ, Muthu S, et al. Safety of switching to nevirapine-based highly active antiretroviral therapy at elevated CD4 cell counts in a resource-constrained setting. J Acquir Immune Defic Syndr 2007;45(5):598- 600. 82. Wit FW, Kesselring AM, Gras L, Richter C, van der Ende ME, Brinkman K, et al. Discontinuation of nevirapine because of hypersensitivity reactions in patients with prior treatment experience, compared with treatment-naive patients: the ATHENA cohort study. Clin Infect Dis 2008;46(6):933-40.
- 141. 133 83. Baylor MS, Johann-Liang R. Hepatotoxicity associated with nevirapine use. J Acquir Immune Defic Syndr 2004;35(5):538-9. 84. Feinberg J. Report from the 16th Conference on Retroviruses and Opportunistic Infections. Lopinavir/r is superior to nevirapine in women who previously received single-dose nevirapine. AIDS Clin Care 2009;21(4):33. 85. Sax PE, Gallant JE, Klotman PE. Renal safety of tenofovir disoproxil fumarate. AIDS Read 2007;17(2):90-2,9-104,C3. 86. Roling J, Schmid H, Fischereder M, Draenert R, Goebel FD. HIV-associated renal diseases and highly active antiretroviral therapy-induced nephropathy. Clin Infect Dis 2006;42(10):1488-95. 87. Cassetti I, Madruga JV, Suleiman JM, Etzel A, Zhong L, Cheng AK, et al. The safety and efficacy of tenofovir DF in combination with lamivudine and efavirenz through 6 years in antiretroviral-naive HIV-1-infected patients. HIV clinical trials 2007;8(3):164-72. 88. Nurutdinova D, Onen NF, Hayes E, Mondy K, Overton ET. Adverse effects of tenofovir use in HIV-infected pregnant women and their infants. Ann Pharmacother 2008;42(11):1581-5. 89. WHO, UNAIDS and UNICEF. Towards universal access: Scaling up of priority HIV/AIDS interventions in the health sector: Progress report 2009 [cited 2009 Nov 11, 2009]: Available from: http://www.who.int/hiv/pub/2009progressreport/en/. 90. Gallant JE, DeJesus E, Arribas JR, Pozniak AL, Gazzard B, Campo RE, et al. Tenofovir DF, emtricitabine, and efavirenz vs. zidovudine, lamivudine, and efavirenz for HIV. N Engl J Med 2006;354(3):251-60. 91. Subbaraman R, Chaguturu SK, Mayer KH, Flanigan TP, Kumarasamy N. Adverse effects of highly active antiretroviral therapy in developing countries. Clin Infect Dis 2007;45(8):1093- 101. 92. McComsey G, Lonergan JT. Mitochondrial dysfunction: patient monitoring and toxicity management. J Acquir Immune Defic Syndr 2004;37 Suppl 1:S30-5. 93. Hawkins C, Achenbach C, Fryda W, Ngare D, Murphy R. Antiretroviral durability and tolerability in HIV-infected adults living in urban Kenya. J Acquir Immune Defic Syndr 2007;45(3):304-10. 94. van Griensven J, Zachariah R, Rasschaert F, Mugabo J, Atte EF, Reid T. Stavudine- and nevirapine-related drug toxicity while on generic fixed-dose antiretroviral treatment: incidence, timing and risk factors in a three-year cohort in Kigali, Rwanda. Trans R Soc Trop Med Hyg 2010; 104(2): 148-53. 95. Kallianpur AR, Hulgan T. Pharmacogenetics of nucleoside reverse-transcriptase inhibitor- associated peripheral neuropathy. Pharmacogenomics 2009;10(4):623-37.
- 142. 134 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach 96. van Griensven J, De Naeyer L, Mushi T, Ubarijoro S, Gashumba D, Gazille C, et al. High prevalence of lipoatrophy among patients on stavudine-containing first-line antiretroviral therapy regimens in Rwanda. Trans R Soc Trop Med Hyg 2007;101(8):793-8. 97. Mutimura E, Stewart A, Rheeder P, Crowther NJ. Metabolic function and the prevalence of lipodystrophy in a population of HIV-infected African subjects receiving highly active antiretroviral therapy. J Acquir Immune Defic Syndr 2007;46(4):451-5. 98. Geddes R, Knight S, Moosa MY, Reddi A, Uebel K, Sunpath H. A high incidence of nucleoside reverse transcriptase inhibitor (NRTI)-induced lactic acidosis in HIV-infected patients in a South African context. S Afr Med J 2006;96(8):722-4. 99. WHO. Antiretroviral therapy for HIV infection in adults and adolescents:Recommendations for a public health approach. 2006. Available from: http://www.who.int/hiv/pub/guidelines/ artadultguidelines.pdf. 100. Tai JH, Udoji MA, Barkanic G, Byrne DW, Rebeiro PF, Byram BR, et al. Pregnancy and HIV disease progression during the era of highly active antiretroviral therapy. J Infect Dis 2007;196(7):1044-52. 101. The antiretroviral pregnancy registry [database on the Internet]. Antiretroviral Pregnancy Registry Steering Committee. 2009. Available from: http://www.apregistry.com/forms/ interim_report.pdf. 102. Peltier CA, Ndayisaba GF, Lepage P, van Griensven J, Leroy V, Pharm CO, et al. Breastfeeding with maternal antiretroviral therapy or formula feeding to prevent HIV postnatal mother-to-child transmission in Rwanda. AIDS 2009;23(18):2415-23. 103. Ouyang DW, Shapiro DE, Lu M, Brogly SB, French AL, Leighty RM, et al. Increased risk of hepatotoxicity in HIV-infected pregnant women receiving antiretroviral therapy independent of nevirapine exposure. AIDS 2009;23(18):2425-30. 104. Musoke P, Guay LA, Bagenda D, Mirochnick M, Nakabiito C, Fleming T, et al. A phase I/II study of the safety and pharmacokinetics of nevirapine in HIV-1-infected pregnant Ugandan women and their neonates (HIVNET 006). AIDS 1999;13(4):479-86. 105. Kunz A, Frank M, Mugenyi K, Kabasinguzi R, Weidenhammer A, Kurowski M, et al. Persistence of nevirapine in breast milk and plasma of mothers and their children after single-dose administration. J Antimicrob Chemother 2009;63(1):170-7. 106. Muro E, Droste JA, Hofstede HT, Bosch M, Dolmans W, Burger DM. Nevirapine plasma concentrations are still detectable after more than 2 weeks in the majority of women receiving single-dose nevirapine: implications for intervention studies. J Acquir Immune Defic Syndr 2005;39(4):419-21. 107. Ribaudo HJ, Haas DW, Tierney C, Kim RB, Wilkinson GR, Gulick RM, et al. Pharmacogenetics of plasma efavirenz exposure after treatment discontinuation: an Adult AIDS Clinical Trials Group Study. Clin Infect Dis 2006;42(3):401-7.
- 143. 135 108. Arrive E, Kyabayinze DJ, Marquis B, Tumwesigye N, Kieffer MP, Azondekon A, et al. Cohort profile: the paediatric antiretroviral treatment programmes in lower-income countries (KIDS-ART-LINC) collaboration. Int J Epidemiol 2008;37(3):474-80. 109. Flys TS, Mwatha A, Guay LA, Nakabiito C, Donnell D, Musoke P, et al. Detection of K103N in Ugandan women after repeated exposure to single dose nevirapine. AIDS 2007;21(15):2077-82. 110. Flys TS, Donnell D, Mwatha A, Nakabiito C, Musoke P, Mmiro F, et al. Persistence of K103N- containing HIV-1 variants after single-dose nevirapine for prevention of HIV-1 mother-to- child transmission. J Infect Dis 2007;195(5):711-5. 111. Wind-Rotolo M, Durand C, Cranmer L, Reid A, Martinson N, Doherty M, et al. Identification of nevirapine-resistant HIV-1 in the latent reservoir after single-dose nevirapine to prevent mother-to-child transmission of HIV-1. J Infect Dis 2009;199(9):1301-9. 112. Coovadia H. Current issues in prevention of mother-to-child transmission of HIV-1. Curr Opin HIV AIDS 2009;4(4):319-24. 113. Coovadia A, Hunt G, Abrams EJ, Sherman G, Meyers T, Barry G, et al. Persistent minority K103N mutations among women exposed to single-dose nevirapine and virologic response to nonnucleoside reverse-transcriptase inhibitor-based therapy. Clin Infect Dis 2009;48(4):462-72. 114. Lockman S, Shapiro RL, Smeaton LM, Wester C, Thior I, Stevens L, et al. Response to antiretroviral therapy after a single, peripartum dose of nevirapine. N Engl J Med 2007;356(2):135-47. 115. Lockman S, McIntyre JA. Reduction of HIV-1 drug resistance after intrapartum single-dose nevirapine. Lancet 2007;370(9600):1668-70. 116. Chi BH, Sinkala M, Stringer EM, Cantrell RA, Mtonga V, Bulterys M, et al. Early clinical and immune response to NNRTI-based antiretroviral therapy among women with prior exposure to single-dose nevirapine. AIDS 2007;21(8):957-64. 117. Lockman S, editor. Lopinavir/ritonavir + tenofovir/emtricitabine is superior to nevirapine + tenofovir/emtricitabine for women with prior exposure to single-dose nevirapine: A5208 (“Octane”). 16th Conference on Retroviruses and Opportunistic Infections; 8-11 February 2009; Montreal, Canada. 118. Coffie PA, Ekouevi DK, Chaix ML, Tonwe-Gold B, Clarisse AB, Becquet R, et al. Maternal 12-month response to antiretroviral therapy following prevention of mother-to-child transmission of HIV type 1, Ivory Coast, 2003-2006. Clin Infect Dis 2008;46(4):611-21. 119. Kuhn L, Semrau K, Ramachandran S, Sinkala M, Scott N, Kasonde P, et al. Mortality and virologic outcomes after access to antiretroviral therapy among a cohort of HIV-infected women who received single-dose nevirapine in Lusaka, Zambia. J Acquir Immune Defic Syndr 2009;52(1):132-6.
- 144. 136 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach 120. McIntyre JA MN, Gray GE, et al. Addition of short course combivir to single-dose viramune for the prevention of mother to child transmission of HIV-1 can significantly decrease the subsequent development of maternal and paediatric NNRTI-resistant virus. 3rd International AIDS Society Conference on HIV Pathogenesis and Treatment; 24-27 July 2005; Rio de Janeiro, Brazil. 121. Chi BH, Sinkala M, Mbewe F, Cantrell RA, Kruse G, Chintu N, et al. Single-dose tenofovir and emtricitabine for reduction of viral resistance to non-nucleoside reverse transcriptase inhibitor drugs in women given intrapartum nevirapine for perinatal HIV prevention: an open-label randomised trial. Lancet 2007;370(9600):1698-705. 122. Van Dyke R JG, Shapiro D, et al. A phase II study of the incidence of nevirapine resistance mutations in HIV-infected Thai women receiving a single intrapartum dose of NVP followed by a postpartum tail of ZDV/ddI or ZDV/ddI/LPV/r: IMPAACT P1032. 16th Conference on Retroviruses and Opportunistic Infections; February 8-11 2009; Montreal, Canada. 2009. 123. Farr S NJ, Ng’ombe T, et al. Addition of 7 days of zidovudine + lamivudine to peripartum single-dose nevirapine effectively reduces nevirapine resistance at 2 and 6 weeks postpartum in HIV-infected mothers. 16th Conference on Retroviruses and Opportunistic Infections; 8-11 February 2009; Montreal, Canada. 124. Lallemant M JG, Ngo-Giang-Huong N, et al. Efficacy and safety of 1-month post-partum zidovudine and didanosine to prevent HIV-1 nevirapine resistance mutations following Intrapartum single-dose nevirapine. 16th Conference on Retroviruses and Opportunistic Infections; 8-11 February 2009; Montreal, Canada. 125. Arrive E, Chaix ML, Nerrienet E, Blanche S, Rouzioux C, Coffie PA, et al. Tolerance and viral resistance after single-dose nevirapine with tenofovir and emtricitabine to prevent vertical transmission of HIV-1. AIDS 2009;23(7):825-33. 126. Marra F Bruno R, Galastri S eds. GP120 induces directional migration of human hepatic stellate cells: a link between HIV infection and liver fibrogenesis. Hepatology 2007. 127. Thio CL, Seaberg EC, Skolasky R (Jr), Phair J, Visscher B, Munoz A, et al. HIV-1, hepatitis B virus, and risk of liver-related mortality in the Multicenter Cohort Study (MACS). Lancet 2002;360(9349):1921-6. 128. Hoffmann CJ, Seaberg EC, Young S, Witt MD, D’Acunto K, Phair J, et al. Hepatitis B and long-term HIV outcomes in coinfected HAART recipients. AIDS 2009;23(14):1881-9. 129. Matthews GV, Avihingsanon A, Lewin SR, Amin J, Rerknimitr R, Petcharapirat P, et al. A randomized trial of combination hepatitis B therapy in HIV/HBV coinfected antiretroviral naive individuals in Thailand. Hepatology 2008;48(4):1062-9. 130. Matthews GV, Seaberg E, Dore GJ, Bowden S, Lewin SR, Sasadeusz J, et al. Combination HBV therapy is linked to greater HBV DNA suppression in a cohort of lamivudine- experienced HIV/HBV coinfected individuals. AIDS 2009;23(13):1707-15.
- 145. 137 131. Baleta A. Trial finds simultaneous HIV/tuberculosis treatment beneficial. Lancet infectious diseases 2008;8(11):669. 132. Middelkoop, ed. Can antiretoviral therapy contain a previously escalating TB epidemic in a high HIV prevalemce community. 5th IAS Conference on HIV Pathogenesis, Treatment and Prevention; 19-22 July 2009; Cape Town, South Africa. 133. Golub JE, Astemborski J, Ahmed M, Cronin W, Mehta SH, Kirk GD, et al. Long-term effectiveness of diagnosing and treating latent tuberculosis infection in a cohort of HIV- infected and at-risk injection drug users. J Acquir Immune Defic Syndr 2008;49(5):532-7. 134. Atun RA, Lebcir RM, Drobniewski F, McKee M, Coker RJ. High coverage with HAART is required to substantially reduce the number of deaths from tuberculosis: system dynamics simulation. Int J STD AIDS 2007;18(4):267-73. 135. Avihingsanon A, Manosuthi W, Kantipong P, Chuchotaworn C, Moolphate S, Sakornjun W, et al. Pharmacokinetics and 48-week efficacy of nevirapine: 400 mg versus 600 mg per day in HIV-tuberculosis coinfection receiving rifampicin. Antivir Ther 2008;13(4):529-36. 136. Chang SY, Lin SW, Hung CC. Do we still need lead-in dosing of nevirapine in HIV-infected patients who are receiving rifampicin-containing antituberculous therapy? Clin Infect Dis 2009;49(9):1452-3; author reply 1453-4. 137. Cohen K, Meintjes G. Management of individuals requiring antiretroviral therapy and TB treatment. Curr Opin HIV AIDS 2010;5(1):61-9. 138. Bhatt EB, Jani IV, Ciaffi L, Luggli M, Bastos R, Samo Gudo P, D. Arakaki, Michon C, Calmy A, Bonnet M, and the ANRS 12146 Study Group, editor. Preliminary safety results of co- administration of nevirapine (NVP) or efavirenz (EFV), and rifampicin (RMP) in HIV- tuberculosis (TB) co-infected patients in Maputo (Mozambique): CARINEMO-ANRS 12146 Trial. 5th IAS Conference on HIV Pathogenesis and Treatment; 2009. 139. la Porte CJ, Colbers EP, Bertz R, Voncken DS, Wikstrom K, Boeree MJ, et al. Pharmacokinetics of adjusted-dose lopinavir-ritonavir combined with rifampin in healthy volunteers. Antimicrob Agents Chemother 2004;48(5):1553-60. 140. Nijland HM, L’Homme R F, Rongen GA, van Uden P, van Crevel R, Boeree MJ, et al. High incidence of adverse events in healthy volunteers receiving rifampicin and adjusted doses of lopinavir/ritonavir tablets. AIDS 2008;22(8):931-5. 141. Rolla VC, da Silva Vieira MA, Pereira Pinto D, Lourenco MC, de Jesus Cda S, Goncalves Morgado M, et al. Safety, efficacy and pharmacokinetics of ritonavir 400mg/saquinavir 400mg twice daily plus rifampicin combined therapy in HIV patients with tuberculosis. Clin Drug Investig 2006;26(8):469-79. 142. L’Homme R F, Nijland HM, Gras L, Aarnoutse RE, van Crevel R, Boeree M, et al. Clinical experience with the combined use of lopinavir/ritonavir and rifampicin. AIDS 2009;23(7): 863-5.
- 146. 138 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach 143. WHO. Prioritizing second-line antiretroviral drugs for adults and adolescents: a public health approach – Report of a WHO working group meeting. Geneva: WHO; 2007. 144. DHHS PoAGfAaADoHaHS. Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents. 2009: Available from: http://www.aidsinfo.nih.gov/ContentFiles/ AdultandAdolescentGL.pdf. 145. Jenny-Avital ER, Joseph K. Rifamycin-resistant Mycobacterium tuberculosis in the highly active antiretroviral therapy era: a report of 3 relapses with acquired rifampin resistance following alternate-day rifabutin and boosted protease inhibitor therapy. Clin Infect Dis 2009;48(10):1471-4. 146. Ebraert H, Salu P. Toxic uveitis caused by pharmacodynamic interactions of Rifabutin and protease inhibitors: a case report. Bull Soc Belge Ophtalmol 2007;(303):57-60. 147. WHO. Operational guide for national tuberculosis control programmes on the introduction and use of fixed-dose combination drugs. 2002: Available from: http://whqlibdoc.who.int/ hq/2002/WHO_CDS_TB_2002.308.pdf. 148. Coutinho A MJ, Ekwaru J, Were W, R Bunnell, Kaharuza F et al. , editor. Utility of routine viral load, CD4 cell count, and clinical monitoring among HIV-infected adults in Uganda: A randomized trial. 15th Conference on Retroviruses and Opportunistic Infections; 3-6 February 2008; Boston, USA. 149. Mugyenyi P WSHJ, Munderi P, Gibb D, Kityo C, et al., eds. Impact of routine laboratory monitoring over 5 years after antiretroviral therapy (ART) initiation on clinical disease progression of HIV-infected African adults: the DART trial final results 2009. 5th IAS Conference on HIV Pathogenesis, Treatment and Prevention; 19-22 July 2009; Cape Town, South Africa. 150. Wilson D, Keiluhu AK, Kogrum S, Reid T, Seriratana N, Ford N, et al. HIV-1 viral load monitoring: an opportunity to reinforce treatment adherence in a resource-limited setting in Thailand. Trans R Soc Trop Med Hyg 2009;103(6):601-6. 151. Keiser O, Tweya H, Braitstein P, Dabis F, Macphail P, Boulle A, et al. Mortality after failure of antiretroviral therapy in sub-Saharan Africa. Trop Med Int Health 2009; 15:2, 251-258 152. Keiser O, MacPhail P, Boulle A, Wood R, Schechter M, Dabis F, et al. Accuracy of WHO CD4 cell count criteria for virological failure of antiretroviral therapy. Trop Med Int Health 2009;14(10):1220-5. 153. Phillips AN, Pillay D, Miners AH, Bennett DE, Gilks CF, Lundgren JD. Outcomes from monitoring of patients on antiretroviral therapy in resource-limited settings with viral load, CD4 cell count, or clinical observation alone: a computer simulation model. Lancet 2008;371(9622):1443-51. 154. Murri R, Lepri AC, Cicconi P, Poggio A, Arlotti M, Tositti G, et al. Is moderate HIV viremia associated with a higher risk of clinical progression in HIV-infected people treated with highly active antiretroviral therapy: evidence from the Italian cohort of antiretroviral-naive patients study. J Acquir Immune Defic Syndr 2006;41(1):23-30.
- 147. 139 155. Cozzi Lepri A, Phillips AN, d’Arminio Monforte A, Castelli F, Antinori A, de Luca A, et al. When to start highly active antiretroviral therapy in chronically HIV-infected patients: evidence from the ICONA study. AIDS 2001;15(8):983-90. 156. Hosseinipour M, van Oosterhout J, Weigel R, Mzigangira D, Saukila N, Mhango B, Phiri R, Phiri S, Kumwenda J and the SAFEST 2 study Team. Validating clinical and immunological definitions of antiretroviral treatment failure in Malawi. 4th IAS Conference on HIV Pathogenesis, Treatment and Prevention; 22-25 July 2009; Sydney, Australia. 157. Fox Z, Dragsted UB, Gerstoft J, Phillips AN, Kjaer J, Mathiesen L, et al. A randomized trial to evaluate continuation versus discontinuation of lamivudine in individuals failing a lamivudine-containing regimen: the COLATE trial. Antivir Ther 2006;11(6):761-70. 158. Sproat M, Pozniak AL, Peeters M, Winters B, Hoetelmans R, Graham NM, et al. The influence of the M184V mutation in HIV-1 reverse transcriptase on the virological outcome of highly active antiretroviral therapy regimens with or without didanosine. Antivir Ther 2005;10(2):357-61. 159. Molina JM, Andrade-Villanueva J, Echevarria J, Chetchotisakd P, Corral J, David N, et al. Once-daily atazanavir/ritonavir versus twice-daily lopinavir/ritonavir, each in combination with tenofovir and emtricitabine, for management of antiretroviral-naive HIV-1-infected patients: 48 week efficacy and safety results of the CASTLE study. Lancet 2008;372(9639):646-55. 160. Ortiz R, Dejesus E, Khanlou H, Voronin E, van Lunzen J, Andrade-Villanueva J, et al. Efficacy and safety of once-daily darunavir/ritonavir versus lopinavir/ritonavir in treatment- naive HIV-1-infected patients at week 48. AIDS 2008;22(12):1389-97. 161. Mills AM, Nelson M, Jayaweera D, Ruxrungtham K, Cassetti I, Girard PM, et al. Once-daily darunavir/ritonavir vs. lopinavir/ritonavir in treatment-naive, HIV-1-infected patients: 96- week analysis. AIDS 2009;23(13):1679-88. 162. Pulido F, Estrada V, Baril JG, Logue K, Schewe K, Plettenberg A, et al. Long-term efficacy and safety of fosamprenavir plus ritonavir versus lopinavir/ritonavir in combination with abacavir/lamivudine over 144 weeks. HIV clinical trials 2009;10(2):76-87. 163. Smith KY, Weinberg WG, Dejesus E, Fischl MA, Liao Q, Ross LL, et al. Fosamprenavir or atazanavir once daily boosted with ritonavir 100 mg, plus tenofovir/emtricitabine, for the initial treatment of HIV infection: 48-week results of ALERT. AIDS Res Ther 2008;5:5. 164. Johnson M, Grinsztejn B, Rodriguez C, Coco J, DeJesus E, Lazzarin A, et al. 96-week comparison of once-daily atazanavir/ritonavir and twice-daily lopinavir/ritonavir in patients with multiple virologic failures. AIDS 2006;20(5):711-8. 165. J Lundgren RP, Worm S, et al. Risk of myocardial infarction with exposure to specific ARV from the PI, NNRTI, and NRTI drug classes: The D:A:D Study. 16th Conference on Retroviruses and Opportunistic Infections; 8-11 February 2009: Montreal, Canada.
- 148. 140 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach 166. S Lang M-KM, Cotte L. Impact of specific NRTI and PI exposure on the risk of myocardial infarction: A case-control study nested within FHDH ANRSC04. 16th Conference on Retroviruses and Opportunistic Infections; Montreal, Canada. 2009. 167. Arribas JR, Pulido F, Delgado R, Lorenzo A, Miralles P, Arranz A, et al. Lopinavir/ritonavir as single-drug therapy for maintenance of HIV-1 viral suppression: 48-week results of a randomized, controlled, open-label, proof-of-concept pilot clinical trial (OK Study). J Acquir Immune Defic Syndr 2005;40(3):280-7. 168. Escobar I, Pulido F, Perez E, Arribas JR, Garcia MP, Hernando A. [Pharmacoeconomic analysis of a maintenance strategy with lopinavir/ritonavir monotherapy in HIV-infected patients]. Enferm Infecc Microbiol Clin 2006;24(8):490-4. 169. Cameron DW, da Silva Barbara A, Arribas Jose R, Myers Robert A, Bellos Nicholaos C, Gilmore N, et al. A 96/Week Comparison of Lopinavir/Ritonavir Combination Therapy Followed by Lopinavir/Ritonavir Monotherapy versus Efavirenz Combination Therapy. J Infect Dis 2008;198(2):234-40. 170. Arribas J. JG, G. Fatkenheuer, M. Nelson, N. Clumeck, F. Pulido et al. The MONET trial: darunavir/ritonavir monotherapy shows non-inferior efficacy to standard HAART, for patients with HIV RNA < 50 copies/mL at baseline. 5th IAS Conference on HIV Pathogenesis, Treatment and Prevention; Cape Town. 2009. 171. C Katlama VM, Algarte-Genin M, Duvivier C, Lambert-Niclot S, Girard PM et al. Efficacy of darunavir/ritonavir as single-drug maintenance therapy in patients with HIV-1 viral suppression: a randomized open-label non-inferiority trial, MONOI-ANRS 136. 5th IAS Conference on HIV Pathogenesis, Treatment and Prevention; Cape Town. 172. Delfraissy JF, Flandre P, Delaugerre C, Ghosn J, Horban A, Girard PM, et al. Lopinavir/ ritonavir monotherapy or plus zidovudine and lamivudine in antiretroviral-naive HIV- infected patients. AIDS 2008;22(3):385-93. 173. Bierman WF, van Agtmael MA, Nijhuis M, Danner SA, Boucher CA. HIV monotherapy with ritonavir-boosted protease inhibitors: a systematic review. AIDS 2009;23(3):279-91. 174. Elliott JH, Lynen L, Calmy A, De Luca A, Shafer RW, Zolfo M, et al. Rational use of antiretroviral therapy in low-income and middle-income countries: optimizing regimen sequencing and switching. AIDS 2008;22(16):2053-67. 175. Evaluation of three strategies of second-line antiretroviral treatment in Africa (Dakar – Bobo-Dioulasso – Yaoundé) (2LADY) [database on the Internet] 2009. Available from: http://clinicaltrials.gov/ct2/show/NCT00928187?term=2LADY&rank=1. 176. Murphy R Sunpath H, Nijhawan A, McLellan M , Kuritzkes D. Lopinavir/ritonavir (LPV/r) + 2 nucleoside analogues as second-line ART in Protease-inhibitor naïve adults in South Africa: Outcomes and adverse effects. 15th Conference on Retroviruses and Opportunistic Infections; 3-6 February 2008; Boston, USA..
- 149. 141 177. M Hull Moore D, Harris M, et al. A lamivudine (3TC)-based backbone in conjunction with a boosted protease inhibitor (PI) is sufficient to achieve virologic suppression in the presence of M184V mutations. 49th Interscience Conference on Antimicrobial Agents and Chemotherapy; 12-15 September 2009; San Francisco, USA. 178. Imaz A, del Saz SV, Ribas MA, Curran A, Caballero E, Falco V, et al. Raltegravir, etravirine, and ritonavir-boosted darunavir: a safe and successful rescue regimen for multidrug- resistant HIV-1 infection. J Acquir Immune Defic Syndr 2009;52(3):382-6. 179. Hicks CB, DeJesus E, Sloan LM, Sension MG, Wohl DA, Liao Q, et al. Comparison of once- daily fos-amprenavir boosted with either 100 or 200 mg of ritonavir, in combination with abacavir/lamivudine: 96-week results from COL100758. AIDS Res Hum Retroviruses 2009;25(4):395-403. 180. Clotet B, Bellos N, Molina JM, Cooper D, Goffard JC, Lazzarin A, et al. Efficacy and safety of darunavir-ritonavir at week 48 in treatment-experienced patients with HIV-1 infection in POWER 1 and 2: a pooled subgroup analysis of data from two randomised trials. Lancet 2007;369(9568):1169-78. 181. Pozniak A, Opravil M, Beatty G, Hill A, de Bethune MP, Lefebvre E. Effect of baseline viral susceptibility on response to darunavir/ritonavir versus control protease inhibitors in treatment-experienced HIV type 1-infected patients: POWER 1 and 2. AIDS Res Hum Retroviruses 2008;24(10):1275-80. 182. Rachlis A, Clotet B, Baxter J, Murphy R, Lefebvre E. Safety, tolerability, and efficacy of darunavir (TMC114) with low-dose ritonavir in treatment-experienced, hepatitis B or C co- infected patients in POWER 1 and 3. HIV clinical trials 2007;8(4):213-20. 183. McKeage K, Perry CM, Keam SJ. Darunavir: a review of its use in the management of HIV infection in adults. Drugs 2009;69(4):477-503. 184. Steigbigel RT, Cooper DA, Kumar PN, Eron JE, Schechter M, Markowitz M, et al. Raltegravir with optimized background therapy for resistant HIV-1 infection. N Engl J Med 2008;359(4):339-54. 185. Cooper DA, Steigbigel RT, Gatell JM, Rockstroh JK, Katlama C, Yeni P, et al. Subgroup and resistance analyses of raltegravir for resistant HIV-1 infection. N Engl J Med 2008;359(4): 355-65. 186. Schiller DS, Youssef-Bessler M. Etravirine: a second-generation nonnucleoside reverse transcriptase inhibitor (NNRTI) active against NNRTI-resistant strains of HIV. Clin Ther 2009;31(4):692-704. 187. Yazdanpanah Y, Fagard C, Descamps D, Taburet AM, Colin C, Roquebert B, et al. High rate of virologic suppression with raltegravir plus etravirine and darunavir/ritonavir among treatment-experienced patients infected with multidrug-resistant HIV: results of the ANRS 139 TRIO trial. Clin Infect Dis 2009;49(9):1441-9.
- 150. 142 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach 188. Llibre JM, Santos JR, Puig T, Molto J, Ruiz L, Paredes R, et al. Prevalence of etravirine- associated mutations in clinical samples with resistance to nevirapine and efavirenz. J Antimicrob Chemother 2008;62(5):909-13. 189. Poveda E, Anta L, Blanco JL, Perez-Elias MJ, Garcia F, Leal M, et al. Etravirine resistance associated mutations in HIV-infected patients failing efavirenz or nevirapine in the Spanish antiretroviral resistance database. AIDS 2010;;24(3 ):469–71.. 190. Geretti AM. Shifting paradigms: the resistance profile of etravirine. J Antimicrob Chemother 2008;62(4):643-7. 191. Sungkanuparph S, Manosuthi W, Kiertiburanakul S, Piyavong B, Chantratita W. Evaluating he role of etravirine in the second-line antiretroviral therapy after failing an initial non- nucleoside reverse transcriptase inhibitor-based regimen in a resource-limited setting. Curr HIV Res 2008;6(5):474-6. 192. Tibotec Theraputics. Dear Healthcare Professional letter. August 2009; Available from http:// www.fda.gov/ForConsumers/ByAudience/ForPatientAdvocates/HIVandAIDSActivities/ ucm180480.htm 193. WHO. Essential prevention and care interventions for adults and adolescents living with HIV in resource-limited settings. 2008. Available from: http://www.who.int/entity/hiv/pub/ prev_care/OMS_EPP_AFF_en.pdf. 194. DiClemente RJ, Wingood GM, Del Rio C, Crosby RA. Prevention interventions for HIV positive individuals. Sex Transm Infect 2002;78(6):393-5. 195. King-Spooner S. HIV prevention and the positive population. Int J STD AIDS 1999;10(3): 141-50. 196. WHO. Priority Interventions HIV/AIDS prevention, treatment and care in the health sector. 2009. 197. Kalichman SC, Cain D, Knetch J, Hill J. Patterns of sexual risk behavior change among sexually transmitted infection clinic patients. Arch Sex Behav 2005;34(3):307-19. 198. Margolin A, Avants SK, Warburton LA, Hawkins KA, Shi J. A randomized clinical trial of a manual-guided risk reduction intervention for HIV-positive injection drug users. Health Psychol 2003;22(2):223-8. 199. Sterk CE, Theall KP, Elifson KW, Kidder D. HIV risk reduction among African-American women who inject drugs: a randomized controlled trial. AIDS Behav 2003;7(1):73-86. 200. WHO. Intensified case finding (ICF), isoniazid preventive therapy (IPT) and TB infection control (IC) for people living with HIV. Report of a Joint World Health Organization, HIV/ AIDS and TB Department meeting. Geneva: 2008.
- 151. 143 201. Walker AS, Ford D, Gilks CF, Munderi P, Ssali F, Reid A, et al. Daily co-trimoxazole prophylaxis in severely immunosuppressed HIV-infected adults in Africa started on combination antiretroviral therapy: an observational analysis of the DART cohort. Lancet 2010;375(9722):1278-86. 202. Mitchell SK, Kelly KJ, Potgieter FE, Moon MW. Assessing social preparedness for antiretroviral therapy in a generalized AIDS epidemic: a diffusion of innovations approach. AIDS Behav 2009;13(1):76-84. 203. Orrell C. Antiretroviral adherence in a resource-poor setting. Curr HIV/AIDS Rep 2005;2(4):171-6. 204. Sodergard B, Hofer S, Halvarsson M, Sonnerborg A, Tully MP, Lindblad AK. A structural equation modeling approach to the concepts of adherence and readiness in antiretroviral treatment. Patient Educ Couns 2007;67(1-2):108-16. 205. Tabarsi P, Saber-Tehrani AS, Baghaei P, Padyab M, Mansouri D, Amiri M, et al. Early initiation of antiretroviral therapy results in decreased morbidity and mortality among patients with TB and HIV. J Int AIDS Soc 2009;12(1):14. 206. Zolopa A, Andersen J, Powderly W, Sanchez A, Sanne I, Suckow C, et al. Early antiretroviral therapy reduces AIDS progression/death in individuals with acute opportunistic infections: a multicenter randomized strategy trial. PLoS ONE 2009;4(5):e5575. 207. Lawn SD, Harries AD, Wood R. Strategies to reduce early morbidity and mortality in adults receiving antiretroviral therapy in resource-limited settings. Curr Opin HIV AIDS 2010;5(1):18-26. 208. WHO. Towards universal access. Scaling up priority HIV/AIDS interventions in the health sector. 2009 Progress Report. 2009. 209. Gray RH, Wawer MJ, Brookmeyer R, Sewankambo NK, Serwadda D, Wabwire-Mangen F, et al. Probability of HIV-1 transmission per coital act in monogamous, heterosexual, HIV-1- discordant couples in Rakai, Uganda. Lancet 2001;357(9263):1149-53. 210. Pao D, Pillay D, Fisher M. Potential impact of early antiretroviral therapy on transmission. Curr Opin HIV AIDS 2009;4(3):215-21. 211. DART Trial Team. Routine versus clinically driven laboratory monitoring of HIV antiretroviral therapy in Africa (DART): a randomised non-inferiority trial. Lancet 2010;375(9709):123-31. 212. Braitstein P, Brinkhof MW, Dabis F, Schechter M, Boulle A, Miotti P, et al. Mortality of HIV- 1-infected patients in the first year of antiretroviral therapy: comparison between low- income and high-income countries. Lancet 2006;367(9513):817-24. 213. Effectiveness of HIV viral load monitoring of patient outcome in resource-poor settings [database on the Internet]2009 [cited Februrary 28, 2010]. Available from: http:// clinicaltrials.gov/ct2/show/NCT00929604?term=Saag&cntry1=AF:ZM&rank=1.
- 152. 144 Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach 214. Monitoring highly active antiretroviral therapy in HIV-infected parentsin Thailand [database on the Internet] 2009 Last Updated: September 14 [cited Frebbrury 18, 2010]. Available from: http://clinicaltrials.gov/ct2/show/NCT00162682?term=Lallemant&cntry1=SE:TH&ra nk=4. 215. Antiretroviral treatment simplified follow-up management assessment (ANRS 12110 STRATALL) [database on the Internet] 2008 Last updated: April 16, 2008. Available from: http://clinicaltrials.gov/ct2/show/NCT00301561?term=Laurent&cntry1=AF:CM&rank=1. 216. Goicoechea M, Liu S, Best B, Sun S, Jain S, Kemper C, et al. Greater tenofovir-associated renal function decline with protease inhibitor-based versus nonnucleoside reverse- transcriptase inhibitor-based therapy. J Infect Dis 2008;197(1):102-8. 217. Mohsen AH, Easterbrook PJ, Taylor C, Portmann B, Kulasegaram R, Murad S, et al. Impact of human immunodeficiency virus (HIV) infection on the progression of liver fibrosis in hepatitis C virus infected patients. Gut 2003;52(7):1035-40. 218. Smit C, van den Berg C, Geskus R, Berkhout B, Coutinho R, Prins M. Risk of hepatitis- related mortality increased among hepatitis C virus/HIV-coinfected drug users compared with drug users infected only with hepatitis C virus: a 20-year prospective study. J Acquir Immune Defic Syndr 2008;47(2):221-5. 219. Benhamou Y, Bochet M, Di Martino V, Charlotte F, Azria F, Coutellier A, et al. Liver fibrosis progression in human immunodeficiency virus and hepatitis C virus coinfected patients. The Multivirc Group. Hepatology 1999;30(4):1054-8. 220. Chen TY, Ding EL, Seage Iii GR, Kim AY. Meta-analysis: increased mortality associated with hepatitis C in HIV-infected persons is unrelated to HIV disease progression. Clin Infect Dis 2009;49(10):1605-15. 221. Mocroft A, Rockstroh J, Soriano V, Ledergerber B, Kirk O, Vinogradova E, et al. Are specific antiretrovirals associated with an increased risk of discontinuation due to toxicities or patient/physician choice in patients with hepatitis C virus coinfection? Antivir Ther 2005;10(7):779-90. 222. Roche. Copegus (ribavirin, USP) prescibing information. 2010. 223. Bani-Sadr F, Denoeud L, Morand P, Lunel-Fabiani F, Pol S, Cacoub P, et al. Early virologic failure in HIV-coinfected hepatitis C patients treated with the peginterferon-ribavirin combination: does abacavir play a role? J Acquir Immune Defic Syndr 2007;45(1):123-5. 224. Rodriguez-Torres M, Torriani FJ, Soriano V, Borucki MJ, Lissen E, Sulkowski M, et al. Effect of ribavirin on intracellular and plasma pharmacokinetics of nucleoside reverse transcriptase inhibitors in patients with human immunodeficiency virus-hepatitis C virus coinfection: results of a randomized clinical study. Antimicrob Agents Chemother 2005;49(10):3997-4008.
- 153. 145 225. Mira JA, Lopez-Cortes LF, Barreiro P, Tural C, Torres-Tortosa M, de Los Santos Gil I, et al. Efficacy of pegylated interferon plus ribavirin treatment in HIV/hepatitis C virus co-infected patients receiving abacavir plus lamivudine or tenofovir plus either lamivudine or emtricitabine as nucleoside analogue backbone. J Antimicrob Chemother 2008;62(6):1365-73. 226. Montes Ramírez ML Rodríguez Zapata M. Report of three cases of hyperlactacidemiae/ lactic acidosis after treatment of hepatitis C with pegylated interferon and ribavirin in HIV coinfected patients Rev Clin Esp 2002;202:543-5. 227. Carrat F, Bani-Sadr F, Pol S, Rosenthal E, Lunel-Fabiani F, Benzekri A, et al. Pegylated interferon alfa-2b vs standard interferon alfa-2b, plus ribavirin, for chronic hepatitis C in HIV-infected patients: a randomized controlled trial. JAMA 2004;292(23):2839-48. 228. Laguno M, Murillas J, Blanco JL, Martinez E, Miquel R, Sanchez-Tapias JM, et al. Peginterferon alfa-2b plus ribavirin compared with interferon alfa-2b plus ribavirin for treatment of HIV/HCV co-infected patients. AIDS 2004;18(13):F27-36. 229. Torriani FJ, Rodriguez-Torres M, Rockstroh JK, Lissen E, Gonzalez-Garcia J, Lazzarin A, et al. Peginterferon Alfa-2a plus ribavirin for chronic hepatitis C virus infection in HIV-infected patients. N Engl J Med 2004;351(5):438-50. 230. Chung RT, Andersen J, Volberding P, Robbins GK, Liu T, Sherman KE, et al. Peginterferon Alfa-2a plus ribavirin versus interferon alfa-2a plus ribavirin for chronic hepatitis C in HIV- coinfected persons. N Engl J Med 2004;351(5):451-9. 231. Laguno M, Cifuentes C, Murillas J, Veloso S, Larrousse M, Payeras A, et al. Randomized trial comparing pegylated interferon alpha-2b versus pegylated interferon alpha-2a, both plus ribavirin, to treat chronic hepatitis C in human immunodeficiency virus patients. Hepatology 2009;49(1):22-31.
- 155. WHO Library Cataloguing-in-Publication Data A guide for adaptation and implementation: revised principles and recommendations: ART for HIV infection in adults and adolescents: recommendations for a public health approach. 1.Anti-retroviral agents - therapeutic use. 2.Anti-retroviral agents - pharmacology. 3.HIV infections - drug therapy. 4.Adult 5.Adolescent. 6.Guidelines. 7.Developing countries. I.World Health Organization. ISBN 978 92 4 159976 4 (NLM classification: WC 503.2) © World Health Organization 2010 All rights reserved. Publications of the World Health Organization can be obtained from WHO Press, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel.: +41 22 791 3264; fax: +41 22 791 4857; e-mail: [email protected]). Requests for permission to reproduce or translate WHO publications – whether for sale or for noncommercial distribution – should be addressed to WHO Press, at the above address (fax: +41 22 791 4806; e-mail: [email protected]). The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement. The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters. All reasonable precautions have been taken by the World Health Organization to verify the information contained in this publication. However, the published material is being distributed without warranty of any kind, either expressed or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall the World Health Organization be liable for damages arising from its use. Printed in Austria
- 156. Antiretroviral therapy for HIV infection in adults and adolescents Recommendations for a public health approach 2010revision AntiretroviraltherapyforHIVinfectioninadultsandadolescentsRecommendationsforapublichealthapproach2010revision Strengthening health services to fight HIV/AIDS HIV/AIDS ProgrammeFor more information, contact: World Health Organization Department of HIV/AIDS 20, avenue Appia 1211 Geneva 27 Switzerland E-mail: [email protected] www.who.int/hiv ISBN 978 92 4 159976 4