2. Goals of the immune system
Prevent entry of pathogen
Prevent growth of pathogen
Kill the pathogen
Eliminate pathogen and repair damage
3. The double edged sword of immune
responses
“Immunitas”:
Freedom from
disease
Protective responses against
infectious agents
“Pathos”:
Suffering/
disease
Host tissue damage
by immune response
4. Immunity
1.Immunity: : Meaning the state of protection from infectious disease.
In 430BC, a plaque in Athens, Those who recovered from the plaque
would not contact the disease a second time.
2. Agents: microorganisms (viruses, bacteria etc) and their products,
foods, chemicals, pollen, tumor cells, etc.
3.Immune system: immune tissues and organs, immune cells, immune
molecules
4.Immune response: collective and coordinated response to the
introduction of foreign substances.
5.Immunology: study the structure of immune system and its
functions.
5. What is the Immune System for?
• Hosts use their IS to maximise survival and reproduction
– Possibly tautological, but true
– The IS does not have the sole aim of killing parasites
• IS is constrained by other physiology
• Persistence of infection does not immediately imply
parasite cunning or immunity failure
• Generate questions about the functions of immunity
– and therefore the mechanisms that might be expected
6. Immunopathology
• For many infections, the immune response
“causes” the disease
– Respiratory syncytial virus
• Eosinophilia creates the clinical disease
• Ablate eosinophilia & mice die without symptoms
– Schistosomiasis
• Circulatory failure due to granuloma formation around eggs
embedded in liver
– Ascaris suum
• Single large dose leads to explusion
• Same dose trickled leads to establishment & little pathology
7. Constraints to Immunity
• IS is expensive in terms of limited resources
(energy & protein)
– Other processes that enhance “fitness”
• E.g. growth & reproduction
– Many physiological processes constrained by
“minimum energy” or “minimum protein”
• IS is dangerous
– Autoimmune disease
8. • Hosts may choose to devote resources to
things other than immunity
– especially if infection is rarely immediately
lethal and continuous (macroparasites)
– not if infection will be lethal if uncontrolled
(viruses)
9. Adaptive Immunity
• Adaptive to overcome pathogen adaptation
– Adaptive to host requirements: protein & energy
• Also adaptive to survival / reproduction context
– Nutrition (resources)
• Malnourished hosts experience more disease
– Gender & Social Status
• Males & females do not have same priorities
• Hormonal influence (effect of testosterone)
– Age
• Priorities change
• Immuno-modulation of parasite burden
10. Ch. 1
Innate – first line of defense
Physical, chemical, inflammatory
barriers
Phagocytic cells
Molecules that recognize certain
classes
of pathogens
Adaptive – specificity, diversity, memory, and
self-nonself recognition
20. Lymphocytes
1.Lymphocytes (except NK cells) are wholly
responsible for the specific immune recognition
of pathogens, so they initiate adaptive immune
responses.
2.Lymphocytes are derived from bone-marrow stem
cells.
3.B lymphocytes develop in the bone marrow.
T lymphocytes develop in the thymus.
22. Antigen presenting cells (APC)
1. Dendritic cells (DC): powerful in antigen processing
and presentation.
2. Macrophage: powerful in antigen processing and
destruction, but low in antigen presentation.
26. Phagocytic cells
¨Monocytes (blood)/Macrophages (tissues)
functions: 1. remove particulate antigens
2. take up, process and present
antigenic peptides to T cells
distribution: Kupffer cells in the liver
microglial cells in the brain
Introduction
28. Phagocytic cells
¨Polymorphonuclear granulocytes
1.neutrophils; basophils; eosinophils
2.neutrophils are short-lived phagocytic cells
multilobed nucleus; 10-20 m
3.neutrophils have a large arsenal of antibiotic
proteins
granules: lysosomes; lactoferrin
30. Tissues and organs of the immune
system
Primary (or central) lymphoid organs
bone marrow
thymus
Secondary (or peripheral) lymphoid organs
spleen
lymph nodes
Mucosal-associated lymphoid tissue (MALT)
31. Mucosal immune system (MIS)
1.non-encapsulated lymphoid tissue in the
lamina propria and submucosal areas of the
gastrointestinal, respiratory and genitourinary
tracts.
2. tonsil, appendix, Peyer’s patches
3. B cell IgA
IEL Adaptive immune ( T cell)
4. function: local (mucosal) immunity
43. Allergies, Autoimmune Diseases
and Graft Rejection
• Response mounted against Ags in the
absence of infectious disease
• Allergy: Ag = innocuous foreign substance
(e.g. pollen)
• Autoimmunity: Ag = self Ag (not tolerant)
• Graft rejection: Ag = foreign cell
• Therapy: Ag-specific suppression and
general immunosuppression
44. Immunodeficiency Diseases
• When some unit or the immune response does not
function effectively
– Can be life threatening
– Often associated with recurrent infections
• Acquired Immune Deficiency Syndrome (AIDS)
– TH1 and TH2 subsets of T cells destroyed
– Caused by human immunodeficiency virus (HIV)
– Individual suffers from multitude of infections,
including those normally controlled by macrophages
#3:Overall theme—fact that immune response can damage tissues
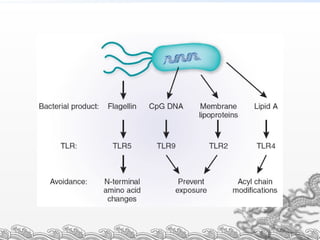
#15:Fig. 1. Models of receptor activation in immune surveillance. A crucial function in host defence is the detection of infection and activation of protective immunity. This function is served by surveillance receptors, such as Toll-like receptors (TLRs). How TLRs detect for infectious microorganisms is unclear. Three models are shown. (a) Self–nonself: the self–nonself model proposes that TLRs on immune cells (right) respond to exogenous or 'nonself` molecules that are derived from microorganisms (left). (b) Danger: the danger model proposes that TLRs on immune cells respond primarily to endogenous molecules released from cells in 'danger`, such as stressful or necrotic cell death, as well as some exogenous molecules. (c) Surveillance: the surveillance model proposes that TLRs on immune cells respond to the degradation of endogenous macromolecules in local microenvironments that coincide with infection and injury, as well as respond to exogenous molecules from microorganisms, and perhaps necrotic cell death.
TLR-TII-24-19-2003