Pharmacotherapy of Drug Abuse or Addiction (Intoxication and Withdrawal Syndrome)
7 likes1,719 views

The document discusses the pharmacotherapy of drug abuse, including definitions of drug abuse, misuse, dependence, and addiction, while highlighting brain areas and neurotransmitter systems involved in addiction. Key concepts such as the reward pathway, the effects of various psychoactive substances, and the management of intoxication and withdrawal are outlined. Treatment strategies for different types of substance abuse and withdrawal symptoms are also presented, emphasizing the importance of pharmacological selection in management.







































Pharmacotherapy of Drug Abuse or Addiction (Intoxication and Withdrawal Syndrome)
- 1. Pharmacotherapy of Drug Abuse Prof. Sawsan Aboul-Fotouh Department of pharmacology, faculty of Medicine, Ain shams University
- 2. 1. Distinguish between drug Abuse, drug misuse and drug dependence. 2. Identify the anatomical areas of the brain involved in the reward (pleasure) pathway 3. Outline the neurotransmitter systems which activate the reward pathway 4. Specify the anatomical areas and receptors involved in activation from psychoactive drugs 5. Predict the anatomical areas and receptors involved in the withdrawal from psychoactive drugs 6. Understand concepts relating to the development of drug addiction. 7. Apply the pharmacological basis for proper selection of the drugs used in the management of intoxication and withdrawal symptoms of substances abuse
- 3. Important Terminologies and Concepts • Drug abuse: Intentional and inappropriate use of a drug resulting in physical, emotional, financial, social & intellectual harmful consequences. e.g. seeking for euphoria or alter perception. • Drug misuse: unintentional or inappropriate use of the prescribed OTC (or using drugs without a prescription). Misuse can include taking a drug in a manner or at a dose that was not recommended by the physician.
- 4. • Drug dependence: A drug is needed to function normally. A. Physical dependence indicates an altered physiological state due to repeated administration of a drug, the cessation of which results in a specific syndrome (Withdrawal Syndrome). Important Terminologies and Concepts
- 5. B. Drug addiction: “Psychological dependence” - Compulsive repeated use of a substance, despite its negative, harmful or dangerous effects. Loss control on taking a Drug. e.g. CVS diseases, cancers with tobacco smoke, -There is Craving. Important Terminologies and Concepts Intense desire to take the drug Craving
- 6. • It is possible to be dependent on a drug without being addicted. e.g. A terminal cancer patient being treated with morphine for pain will experience withdrawal if the drug is stopped, but they are not a compulsive user of the drug therefore they are not addicted.
- 7. Tolerance: Drug response after continuous use Need larger dose to produce the same initial effect loss of control of addict over amount of drug used.
- 10. Drug Group Most Common Other Examples I. CNS Depressants A.Opioids B. Sedative hypnotics • Heroin • Morphine • Codeine • Meperidine • Hydromorphone • Ethanol or Alcohols • Benzodiazepines • Rohypnol© (Flunitrazepam) • Barbiturates • Nonbarbiturate sedatives (Lyrica) II. CNS Stimulants • Cocaine • Methamphetamine (Ice) • MDMA or Ecstasy (Hallucinogen) • Amphetamines • Methylphenidate • Nicotine, Khat (Cathinone) III. Hallucinogens psychedelics • Lysergic acid diethylamide (LSD) • Dimethyltryptamine (DMT) • Phencyclidine (PCP) • Ketamine • Psilocybin, Ayahuasca • Mescaline (peyote cactus), IV. Cannabinoids • Hashish, cannabis, Marijuana • Bhango, Weed • Synthetic (Voodoo and Strox) V. Inhalants (hallucination &euphoria) VI. Others • (solvents glue & Paint) • OTC Cough/Cold Medicines (Dextromethorphan ) • Steroids (Anabolic) • Nitrous oxide, Ether • Anticholinergics -Benztropine & Trihexyphenidyl tablets - Cyclopentolate & Tropicamide eye drops
- 12. Reward (Pleasure) Pathway (plays a key role in addiction) 1. Nucleus accumbens (NAc) = Pleasure center 2. Ventral tegmental area (VTA) 3. Prefrontal cortex (PFC) Pleasure center ↑ ↑Dopamine in NAc →Euphoria NAc
- 13. TYPES OF REWARD SYSTEMS A. NATURAL reward stimulus (e.g., food, water, sex, ….) B. ARTIFICIAL reward stimulus (e.g., drugs as heroin, Hashish ……), information travels from VTA to NAc & then to PFC. VTA contains dopamine (DA) neurons which release DA in the nucleus accumbens →Euphoria and in the prefrontal cortex (Behavior)
- 14. Drugs Act in Different Parts of Reward pathway • Heroin, Alcohol, Hashish (Cannabis) & nicotine (Tobacco) act on the VTA stimulating the dopaminergic neuron cell body to release DA in the NAc →↑ DA in NAc →Euphoria. • Alcohol induce euphoria via release of endogenous opioids in VTA • BZD also stimulate DA neurons in VTA & enhance euphoric effect of other substances Heroin, Alcohol, Hashish &nicotine
- 15. • Amphetamines and Cocaine act directly on NAc DA nerve terminal to stimulate release and/or inhibit the reuptake of DA→↑ DA in NAc→ Euphoria Drugs Act in Different Parts of Reward pathway Amphetamines Cocaine
- 17. • In all rewards, dopamine is the final activation chemical that induce euphoria when increased in the NAc ↑↑Dopamine
- 18. REWARD DEFICIENCY • Prolonged drug use → neurodegeneration of DA neurons in the reward pathway → chronic feelings of anxiety, depression & an inability to feel good. • And ↓ DA in NAc → development of craving. • The person can only feel normal when under the influence of the drug and developed negative and positive reinforcement. 18
- 19. Negative reinforcement Escape and avoidance of negative affect is the motive for addictive drug use Positive reinforcement Pleasurable sensations associated with a taking the drug or addiction behavior, motivating the person to repeat drug intake.
- 20. Withdrawal: Corticotrophin Releasing Factor (CRF) affective & somatic symptoms Heart rate Blood pressure Blood glucose Response to stressors Key elements CRF and NE neurons in the amygdala
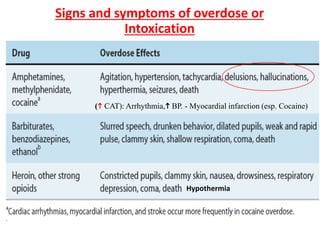
- 21. Signs and symptoms of overdose or Intoxication Hypothermia ( CAT): Arrhythmia, BP. - Myocardial infarction (esp. Cocaine)
- 22. Signs and symptoms of Withdrawal from selected drugs of abuse Body aches Sympathetic overactivity, hyperthermia Very Strong Craving w Cocaine Delirium Tremens
- 23. Alcohol (Strong Dependence) Mechanism : enhances GABA-A receptor action (cross tolerance with BZDs), ↓glutamate, release endogenous opioids (euphoric effect). Acute Effects • Euphoria - relaxation - increased self-confidence. Withdrawal Syndrome • Similar to barbiturates with delirium tremens: delirium - tremors - psychosis (visual hallucinations of crawling bugs). Chronic Abuse (Alcoholism) 1. Withdrawn, homicidal or suicidal individual - work & family problems. 2. Liver cirrhosis - peptic ulcer – cardiomyopathy. 3. Dementia - peripheral neuropathy. 4. ↓↓Thiamine (Vit. B1) Wernicke-Korsakoff syndrome (Ophthalmoplegia, ataxia, confusion, psychosis).
- 24. Ophthalmoplegia + Ataxia + Confusion Psychosis + Amnesia (Wernicke’s encephalopathy) (Korsakoff’s syndrome)
- 25. Nicotine (Very Strong Craving) Mechanism : acts on central α4β2 nicotinic Ach receptors in VTA → ↑DA in NAc reward pathway → reward upon smoking → dependence. Acute Effects: euphoria - anxiety - concentration -appetite Chronic Abuse: cancer, lung diseases, ischemic heart diseases. Withdrawal Syndrome: Insomnia - Anxiety – aggression- Depression - appetite.
- 26. Lysergic Acid Diethylamide (LSD) (Other hallucinogens: DMT, PCP…..) • Taken recreationally not regularly no dependence ??? (NIDA) Acute Effects • Euphoria & sensory changes: sights & sounds are distorted & fantastic. • Hallucinations, delusions, illusions, Philosophical & creative thinking. Risk of LSD Bad trips: frightening hallucinations homicide or suicide. Persistent Psychosis and flashbacks are two long-term effects of Hallucinogens.
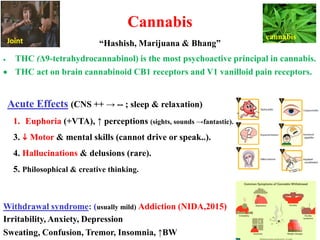
- 27. Cannabis “Hashish, Marijuana & Bhang” • THC (Δ9-tetrahydrocannabinol) is the most psychoactive principal in cannabis. • THC act on brain cannabinoid CB1 receptors and V1 vanilloid pain receptors. Acute Effects (CNS ++ → -- ; sleep & relaxation) 1. Euphoria (+VTA), ↑ perceptions (sights, sounds →fantastic). 3. Motor & mental skills (cannot drive or speak..). 4. Hallucinations & delusions (rare). 5. Philosophical & creative thinking. Withdrawal syndrome: (usually mild) Addiction (NIDA,2015) Irritability, Anxiety, Depression Sweating, Confusion, Tremor, Insomnia, ↑BW cannabis Joint
- 28. Risks of Cannabis Abuse 1. Academic failure & ↓achievement& life outcomes 2. Psychosis (Hallucination, delusions “Schizophrenia”) 3. Motor Deficits:↓ Cerebellar Metabolism 4. Amotivational syndrome. 5. The immune system impaired. 6. Sexual & reproductive Dysfunction: -Male: ↓ testosterone, sperm count& ability, libido -Female: inhibition of ovulation. In Pregnancy: miscarriage and ectopic pregnancy
- 29. Management of Acute Intoxication in substance Abuse
- 30. Management of Acute Intoxication in substance Abuse 1. Correction of life-threatening symptoms: (ABC) 2. Prevention absorption: 3. Facilitate removal -Alkalinization (Na Hco3) of urine with Barbiturates (acidic PKa) -Acidification (As. a, NH4Cl) , of urine with Amphetamine (basic PKa) -Forced diuresis ,Peritoneal dialysis, hemodialysis
- 31. 4. Antidote (if present): -Naloxone in Heroin intoxication -Flumazenil in Benzodiazepine intoxication -In Alcohol Intoxication: ▪ IV glucose to correct hypoglycemia (acute pancreatitis). ▪ Thiamine 100 mg IV or IM (to prevent neurologic injury) 5.Haloperidol and /or Midazolam injection for Agitation and psychosis (e.g. in stimulants, Hallucinogens, Alcohols…) Management of Acute Intoxication in substance Abuse
- 32. LSD (DMT, PCP…) Abuse • Calm the patient during bad trips. 1-long-lasting benzodiazepines, e.g. diazepam, clonazepam 2-Anticonvulsants valproate & carbamazepine (Mainly anti-impulsivity) 3-Antipsychotic agents for hallucinogen-induced psychosis, Management of Acute Intoxication in substance Abuse
- 33. Management of Withdrawal Syndrome in substance Abuse
- 34. Short-acting agents have More abuse & More Withdrawal syndrome than that following longer-acting agents.
- 35. I. symptomatic treatments: e.g. Ibuprofen for Body aches, -promethazine for nausea & vomiting, -diphenhydramine for sleep. -Mirtazepine as antidepressant and hypnotic. Ramelteon hypnotic - Haloperidol injection for Agitation and psychosis II. Anti-impulsivity Drugs: SSRIs e.g. Fluoxetine & antiepileptics e.g. valproate, carbamazepine Management of Withdrawal Syndrome in substance Abuse
- 36. III. α2 Agonists if sympathetic overactivity e.g. Clonidine especially in Heroin withdrawal. IV. Specific strategies in: A- Heroin abuse: (see Opioids) Detoxification (by Methadone or Buprenorphine) and then Maintenance (on Naltrexone). B- Barbiturates and BZDs abuse: Replace short-acting agent by a longer-acting one less severe withdrawal: Phenobarbital for pentobarbital. Diazepam for clonazepam, alprazolam, flunitrazepam. Management of Withdrawal Syndrome in substance Abuse (cont.)
- 37. C- Tobacco (Nicotine) abuse: 1.Nicotine replacement : nicotine gum - transdermal patch - inhaler – nasal spray. 2. Bupropion: ↑DA →↓ craving & Blocks α4β2 nAch R→ ↓ Relapse. 3.Varenicline : partial agonist at CNS α4β2 nicotinic Ach receptors → partial stimulation while competitively inhibiting nicotine binding → blocks ability of nicotine to stimulate VTA DA system→ ↓ craving & withdrawal syndrome. Management of Withdrawal Syndrome in substance Abuse (cont.)
- 39. D- Alcohol Withdrawal: (Delirium Tremens) 1. Diazepam Replaces alcohol and Anticonvulsant 2. Thiamine (V.B1) supplements. 3. Drugs ↓Relapse: a. Disulfiram (Antabuse) b. Naltrexone (Block opioid receptors) c. Acamprosate (↓craving) Management of Withdrawal Syndrome in substance Abuse (cont.)
- 40. Inhibits metabolism step II aldehyde dehydrogenase accumulation of acetaldehyde nausea & vomiting & flushing (disulfiram -like reaction). → patients stop drinking. ↓↓ ✓ ++ GABA-A ✓ Opioid antagonist ✓ ↑ 5-HT
- 41. E- Cocaine and Amphetamine abuse Bupropion ( craving & TTT depressive symptoms of withdrawal). N.B. chemical structure of bupropion is similar to amphetamine. F- Hashish (Marijuana or Cannabis) Abuse ▪ Naltrexone ▪ Dronabinol (synthetic cannabinoid used as antiemetic) NIDA 2019: PCP can be addictive (cravings, headaches, and sweating are withdrawal symptoms) & No specific ttt till Now Management of Withdrawal Syndrome in substance Abuse (cont.)