



























Practical Clinical refraction class 3.pptx
- 1. Practical Clinical Refraction (Optics Class 3) Dr. Shahrina Mahfooz MRCSEd (Ophth), FICO (UK), FCPS,MCPS Long Term Fellowship in Cataract Surgery Long Term Fellow Pediatric Ophthalmology & Strabismus, IIE&H
- 2. Introduction • Experienced refractionists know that prescribing is an art as well as a science.
- 3. History • The patient's age and occupation and special visual requirements, e.g. occupation and hobbies, must be ascertained. • Visual symptoms, eye-related diseases and family history of eye disease, especially glaucoma, must be enquired for. • The patient's past history of spectacle wear is important, and it is wise to find out the previous prescription, if this is available, and to examine the old glasses.
- 4. Cont. • Note the lens form of the previous glasses. Myopes are especially intolerant of a change in lens form and some prefer to continue wearing plano-concave lenses, known as 'flats', even though this may not be the best form of lens for their prescription. Notice the type of multifocal lenses in use and whether the patient is happy with them.
- 5. Examination • The visual acuity is measured uniocularly for distance and near, unaided and with existing spectacles. • Fog the fellow eye of patients with nystagmus with a high plus lens as complete occlusion makes the nystagmus worse and lowers the uniocular acuity. • If the acuity is very poor, examine briefly with the ophthalmoscope at this stage to exclude a pathological cause. • More detailed scrutiny of the fundi should be left until after the refraction to avoid photostress-induced reduction of acuity.
- 6. Objective Refraction • Perform the cover/uncover test to detect any manifest squint. If the patient has a manifest squint without diplopia, binocular vision is lacking and it will not be possible to test the muscle balance by the Maddox rod and wing tests which depend on binocular vision. • Fit the trial frame, taking care that the lens apertures are centred on the pupils with the patient gazing straight ahead. • Remember always to place high power trial lenses in the back cell of the trial frame
- 7. Cont. • Perform the retinoscopy with the patient gazing at a distant object, such as the top letter of the test type. • It is important to perform the retinoscopy as close to the patient's visual axis as possible in order to measure the true optical length of the eye. Care should be taken to ensure that the patient's view of the distant fixation object is not obstructed. To this end the examiner should ideally use his right eye to examine the patient's right eye and his left eye for the patient's left eye. If the examiner does get in the way, the patient loses distant fixation and may start to accommodate • In the presence of manifest squint the dominant eye may have to be occluded to achieve steady fixation with the non-dominant eye.
- 8. • In the case of young children, or children who have a latent or manifest squint, the ciliary muscle should be paralysed with a topical cycloplegic drug before retinoscopy is performed. • This allows the true magnitude of any refractive error to be determined
- 9. • Some refractionists place a plus lens of the dioptric value of their working distance (e.g. +1.50 DS for 2/3 metre) in the trial frame before commencing the retinoscopy. Once the point of reversal or neutral point has been reached for both eyes, this lens is removed and the subjective examination started with the lenses remaining in the frame
- 10. Cont. • After viewing the retinoscopy reflex through the working distance lens, further spherical lenses are added, convex if the movement is 'with' and concave if 'against' (Fig. 16.1a-c) until the neutral point is reached in one meridian (Fig. 16.1d). • Cylindrical lenses may then be used to neutralise the other meridian and to find the axis of the astigmatism present.
- 11. • The same method may also be used to identify the axes of astigmatism if spherical lenses alone are used during retinoscopy, e.g. during cycloplegic retinoscopy of a small child when it is easier to hold lenses in the hand rather than use a trial frame. The reflex in the pupil will only align with the streak when both lie in one principal meridian of astigmatism (Fig. 16.1d-e).
- 12. • The retinoscopy findings are usually recorded in the UK according to the following convention
- 13. • A cross is drawn in the orientation of the principal meridians, and the angle of one meridian marked. The dioptric value of the point of reversal is marked on each meridian and the working distance recorded. If this result is transposed into a lens prescription (corrected for working distance) the axis of any cylinder lies at 90° to the line of its meridian.
- 14. • If the refraction varies between the central and peripheral parts of the pupillary aperture, there may be an increase in brightness in the centre or periphery due to spherical aberrations. • For example, in nucleosclerosis the central zone is relatively myopic compared with the periphery and the centre of the pupil appears bright. To judge the end-point • which may not be as sharply defined as usual, concentrate on the central zone in which the visual axis lies
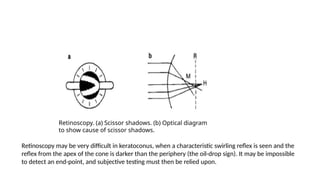
- 15. Oblique Astigmatism • It is sometimes difficult to decide whether the reflex is moving 'with' or 'against' the movement of the retinoscope because there appear to be two reflexes in the pupil, moving towards and away from each other like the blades of a pair of scissors, so-called 'scissor shadows’. • This is due to a difference in refraction between different zones of the pupillary aperture. It is more commonly seen with a dilated pupil and near the end-point of retinoscopy, when one area will be relatively myopic, M, while the other is relatively hypermetropic, H, to the plane of observation, R . • It is traditionally taught that the end-point is taken when the two reflexes meet in the centre of the pupil, but this may be difficult to judge.
- 16. Retinoscopy. (a) Scissor shadows. (b) Optical diagram to show cause of scissor shadows. Retinoscopy may be very difficult in keratoconus, when a characteristic swirling reflex is seen and the reflex from the apex of the cone is darker than the periphery (the oil-drop sign). It may be impossible to detect an end-point, and subjective testing must then be relied upon.
- 17. Subjective Refraction • Make the correction for your working distance (add -1.50 DS for 2/3 metre or remove the 'working distance lens’ if one was used) and, because patients usually do not tolerate the full cylindrical correction, it helps to reduce the cylinder by approximately a quarter of its value before commencing the subjective examination. • Occlude the fellow eye (unless nystagmus is present, in which case use a fogging technique)
- 18. • Using the distance test type, first verify the sphere by offering small plus and minus additions until no further improvement can be made. Patients with good visual acuity can appreciate a difference of 0.25 DS while those with poor acuity may only appreciate larger increments, e.g. 0.50 DS. Next verify the axis of the cylinder before adjusting its power . • If a large change is found in the cylinder, it is wise to go back and recheck the sphere. If the patient is myopic, the duochrome test should be done monocularly and binocularly.
- 19. • If the red letters are only marginally clearer than the green when the patient views them monocularly, the green letters may be clearer when the eyes are used together. A small reduction, e.g. +0.25 DS, to one or both eyes may be needed to make the red letters clearer binocularly and ensure that the patient will be comfortable, and not accommodating, when wearing the prescription
- 20. Cont. • Record the prescription and acuity for each eye, and the binocular acuity. Remember to measure and record the back vertex distance (BVD) if the power of the spherical lens exceeds 5 dioptre. • Such a lens should be in the back cell of the trial frame and the BVD may be conveniently judged using a ruler held beside the arm of the trial frame whilst viewing the patient from the side.
- 21. • Use the Maddox rod to check the muscle balance for distance. Some patients are initially unable to see the white spotlight and the red line, especially if there is confusing side illumination in the room. Occlude each eye in turn to ascertain that the spot and line are visible to the appropriate eye uniocularly, and then uncover both eyes and see if the patient is able to perceive them simultaneously. If the patient sees them one at a time uniocularly but not simultaneously with both eyes uncovered, his binocular vision must be defective or absent.
- 24. Cont. • If the patient is presbyopic, calculate the likely reading addition and add this to the distance lenses in the trial frame. In practice the reading addition is estimated by rule-of-thumb from the patient's 'age: • 45-50 years - +1.00 D addition • 50-55 = +1.50 D addition • 55-60 - +2.00D addition • over 60 = +2.50 D addition • In normal circumstances not more than +2.50 DS addition should be given. However, pseudophakic patients often prefer a +3.00 DS addition. Record the near acuity for each eye alone and binocularly.
- 25. Image Distortion • Use the Maddox wing to check the near muscle balance. Orthophoria for distance but a large exophoria for near indicates convergence insufficiency. • This may cause such symptoms as headache or eye-strain after close work, or it may be asymptomatic. • If the patient has symptoms, the convergence should be strengthened by means of convergence exercises. If base-in prisms are prescribed, the convergence may become weaker still, and progressively stronger prisms will be required. Vertical muscle imbalances for near may require prismatic correction, but again the full value of prism is rarely required or tolerated.
- 26. Measurement of Interpupillary Distance • It is sometimes useful to measure the patient's interpupillary distance. • The measurement of the interpupillary distance is important in babies and small children, especially if high power lenses have been prescribed, as decentration caused by an unsuitable spectacle frame will introduce an unwanted prismatic effect. • Poor centration of aphakic spectacle lenses also causes an unwanted prismatic effect and this is a common cause of intolerance of aphakic glasses.
- 27. • The anatomical interpupillary distance may be measured by the following methods. A millimetre rule is rested across the bridge of the patient's nose and the patient asked to look at the examiner's left eye. The zero of the rule is aligned with the nasal limbus of the patient's right eye (which will be looking straight ahead at the examiner's left eye). The patient is then instructed to look at the examiner's right eye and the position of the temporal limbus of the patient's left eye is noted, giving the anatomical interpupillary distance. (The measurements are taken from limbus to limbus to exclude inaccuracy due to differences or changes in pupil size.) • Alternatively, a fixation light may be held in front of each of the examiner's eyes in turn and a similar procedure followed, the distance between the corneal light reflexes on the patient's eyes being measured.
- 28. Some tips • Do not change the axis of the cylinder, especially in a myope, unless there are compelling reasons for doing so. • Do not change the lens form worn by a myope. • Do not prescribe a large cylinder for any patient who has never worn a cylindrical correction before. Break them in gradually. The exception to this is pseudophakic patients who tolerate a full astigmatic correction well. • Do not overcorrect hypermetropes: better to leave them 0.25 DS undercorrected so they can read the bus numbers in the far distance
- 29. • Do not fully correct myopes: better to leave them 0.25 DS undercorrected so they do not have to use their accommodation for distance. • Do not give too great a reading addition, so the patient cannot read the newspaper held at arm's length . • Do not recommend bifocal or progressive lenses without carefully considering the needs, occupation and frailties of the patient. • Discuss with the patient the subjective and practical points relevant to the new prescription, e.g. warn a new bifocal wearer to be careful at steps.
- 30. • Do not alter a satisfactory prescription unless there is a very definite reason to do so. • Do not advise patients to buy new glasses because of a minor change in prescription that they will not be able to appreciate subjectively.